Pectoralis major
Biceps brachii – long head
Coracobrachialis
Pectoralis major
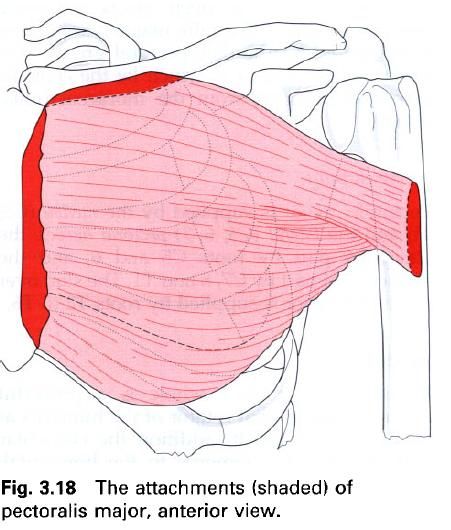
Pectoralis major is found on the upper half of
the anterior surface of the thoracic wall. It is a thick triangular muscle with
clavicular and sternocostal parts, which may be separated by a groove, although
they are usually continuous with each other. On their way to the humerus, the twisting fibres of
pectoralis major from the rounded anterior fold of the axilla.
The smaller, clavicular attachment of
pectoralis major is from the medial half
of the anterior surface of the clavicle; the larger, sternocostal
attachment comes from the anterior
surface on the manubrium and body of the sternum, the anterior aspects of the upper six costal cartilages, the anterior part of the sixth rib as well as the aponeurosis of
the external oblique muscle of the
abdomen.
From this large central attachment, the muscle
narrows and inserts via a laminated tendon into the lateral hip of the intertubercular
groove of the humerus. The
anterior lamina, which comprises the clavicular part of the muscle, runs to the
lower part of the humeral attachment. Fibres from the sternocostal part of the
chest wall form the posterior lamina, which passes upwards behind the anterior
lamina to the upper part of the attachment of the muscle to the humerus. In this way the tendon comes to
resemble a U in cross-section. The posterior part blends with the shoulder
joint capsule, while the anterior, clavicular fibres blend with the attachment
of deltoid.
As the most superficial of the muscles of the
anterior thoracic wall, pectoralis major lies on top of pectoralis minor, the ribs and serratus anterior. In the female, the muscle is covered by the breast; indeed the
fibrous septa of the breast are attached to the deep fascia overlying
pectoralis major. Pectoralis major is separated from deltoid by the deltopectoral groove(the infraclavicular fossa) in
which lie the cephalic vein and branches from the thoracoacromial artery.
Nerve
supply
Pectoralis major is supplied by the medial(C8, T1) and the lateral(C5, 6, 7) pectoral nerves; the clavicular part by roots C5 and 6, and the
sternocostal part by C7, 8 and T1. The skin over pectoralis major is supplied by
roots T2 to T6.
Action
Pectoralis major as a whole is a powerful
adductor and medial rotator of the humerus
at the shoulder joint. In addition to the clavicular part can flex the humerus to the horizontal, while the
sternocostal fibres, because of their direction, can extend the flexed humerus, particularly against resistance
to the anatomical position. With the humerus
fixed, as in gripping a bed table or chair back, pectoralis major pulls on the
upper ribs to assist inspiration during respiratory distress.
Functional
activity
Pectoralis major is one of the major climbing
muscles, so that if the arms are fixed above the head, the massive power of the
muscle can be used to pull the trunk upwards. It is assisted in this activity
by latissimus dorsi. In pushing, punching and throwing movements, pectoralis
major acts to move the humerus
forwards forcefully, whilst serratus anterior and pectoralis minor
simultaneously protract the pectoral girdle.
In exercises, such as the “press-up”,
pectoralis major contracts concentrically on the upward movement and
eccentrically on the downward pressure. The sternocostal part is best palpated
if this same position is maintained against an upward pressure. The integrity
of the muscle can be tested by adduction of the arm against resistance.
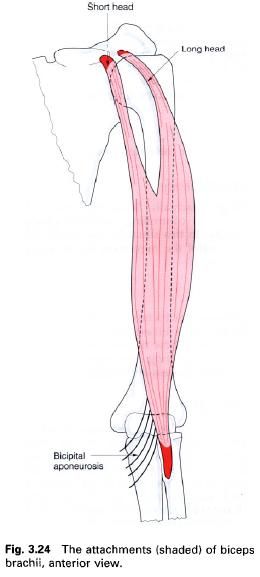
Biceps brachii
Biceps brachii is a prominent fusiform muscle
on the anterior aspect of the arm. It arises by two tendinous heads as its
upper end, and attaches by one tendinous heads at its upper end, and attaches
by one tendinous insertion at its lower end. The upper end is covered by deltoid and pectoralis major, but the
main part of the muscle is only covered by skin and subcutaneous fat.
The short head of biceps brachii arises by a
flat tendon, shared with coracobrachialis, from the apex of the coracoid process
of the scapula. The long head arises
from the supraglenoid tubercle of the
scapula and the adjacent glenoid labrum of the shoulder joint.
The tendon of the long head runs within the shoulder joint wrapped in a
synovial sleeve and leaves to enter the intertubercular groove by passing deep to the transverse humeral ligament. The two
fleshy bellies continue towards the elbow with the two heads fusing to form
with the two heads fusing to form a single muscle just below the middle of the
arm. At the elbow, a single flattened tendon is formed which twists through 90°
before attaching to the posterior part
of the radial tuberosity. A bursa
separates the tendon from the remainder of the radial tuberosity. The prominent
bicipital aponeurosis, a strong
membranous band arising from the lateral side of the main tendon, runs
downwards and medially across the cubital fossa, in front of the brachial
artery and median nerve, to attach to the deep fascia on the ulnar side of the
forearm.
Nerve
supply
Biceps brachii is supplied by the musculocutaneous nerve, root value C5,
and 6. The skin over biceps is supplied by the roots C5, 6, T2 and T3.
Action
Biceps brachii is not only an important flexor
of the elbow joint, but also a powerful supinator of the forearm. Often these
two actions are performed together with any unwanted actions being cancelled by
antagonists. Maximum power is achieved for both flexion and supination with the
elbow at 90°. When the elbow is fully extended the supinating action of biceps
is lost. Biceps is also a flexor of the shoulder joint, and the fact that the
long head crosses the superior part of the joint means that it has an important
stabilizing role.
Functional
activity
Biceps may use its supinatory and flexing
actions sequentially in an activity, as, for example, in inserting a corkscrew
and pulling out the cork. During this activity the head of the ulna may move medially due to the force
of the biceps contraction transmitted to its posterior border via the bicipital
aponeurosis.
When deltoid is paralysed, the long head of
biceps can be re-educated to abduct the shoulder. This is accomplished by
laterally rotating the humerus at the
shoulder joint in order to put the long head into a more appropriate position.
Palpation
With the elbow flexed to 90° and the forearm
pronated, the muscle can be felt contracting in the middle of the arm when
supination against resistance is attempted.
The lower part of the muscle is easily palpated
through the skin. Proximally, each tendon may be palpated but with some degree
of difficulty. The tendon of the long head lies between the two tubercles.
Having determined these, firm deep pressure between them is needed to locate
the tendon. This is the point at which deep transverse frictions or electrical
treatments are applied when the tendon becomes inflamed.
The short head can be found by first palpating
the apex of the coracoid process, and then placing the fingers just below it.
As the elbow is flexed, the tendon can be felt to stand out.
At the elbow, the tendon of insertion is best
palpated with the elbow flexed to 20°. In this position it can be easily
gripped between the index finger and thumb. If, in this same position, the
subject is asked to resist a strong downward pressure on the forearm, the upper
border of the bicipital aponeurosis can be seen and felt as a crescentic border
running downwards and medially from the main tendon.
The tendon of biceps is the point at which the
biceps reflex is tested, often by the examiner placing his or her thumb over
the tendon and then tapping it with a patella hammer. The resultant reflex
contraction can be felt below the thumb and biceps may be seen contracting if
the reflex is brisk enough.
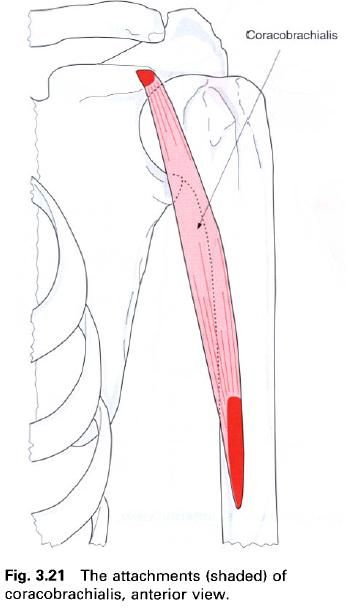
Coracobrachialis
Coracobrachialis is the only true
representative in the arm of the adductor group of muscles found on the leg. It
arises via a rounded tendon, in conjunction with the short head of biceps
brachii, from the apex of the coracoid process of the scapula and attaches by a flat tendon to
the medial side of the shaft of the humerus at about its midpoint,
between triceps and brachialis. Some fibres may continue into the medial
intermuscular septum of the arm.
Nerve
supply
Coracobrachialis is usually supplied by the musculocutaneous nerve as it pierces the
muscle, root value C6, 7. However, the nerve to coracobrachialis may arise
directly from the lateral cord of the brachial plexus. The skin over the muscle
is supplied by roots T1 and T2.
Action
Coracobrachialis is an adductor and weak flexor
of the arm at the shoulder joint.
Palpation
Coracobrachialis can be seen and felt as a
rounded muscular ridge on the medial side of the arm when it is fully abducted
and then adducted against resistance.