



Cartilage
Cartilage is supplementary to bone, being
formed wherever strength, rigidity and some elasticity are required. In fetal
development, cartilage is often a temporary tissue being later replaced by
bone. However, in many places cartilage persists throughout life. Although a
rigid tissue, cartilage is not as hard or strong as bone. It is also relatively
non-vascular being nourished by tissue fluids. A vascular invasion of cartilage
often results in the death of the cells during the process of ossification of
the cartilage and its eventual replacement by bone. Except for the articular
cartilage of synovial joints, cartilage possesses a fibrous covering layer, the
perichondrium.
There are three main types of cartilage: hyaline cartilage, white fibrocartilage and
yellow fibrocartilage.
Hyaline cartilage
This forms the temporary skeleton of the fetus
from which many bones develop. Its remnants can be seen as the articular
cartilages of synovial joints, the epiphyseal growth plates between parts of an
ossifying bone during growth, and the costal cartilages of the ribs. At
joint surfaces it provides a certain degree of elasticity to offset and absorb
shocks, as well as providing a relatively smooth surface permitting free
movement to occur. With increasing age, hyaline cartilage tends to become
calcified and sometimes ossified.
White fibrocartilage
White fibrocartilage contains bundles of white
fibrous tissue which give it great tensile strength combined with some
elasticity so that it is able to resist considerable pressure. It is found at
many sites within the musculoskeletal system: 1) within the intervertebral discs between adjacent vertebrae; 2) in
the menisci of the knee joint; 3) in the labrum deepening the glenoid fossa of
the shoulder joint and the acetabulum of the hip joint; 4) in the articular
discs of the wrist, sternoclavicular, acromioclavicular and temporomandibular
joints, and 5) as the articular covering of bones which ossify in membrane,
e.g. the clavicle and mandible.
White fibrocartilage may calcify and ossify.
Yellow fibrocartilage
Yellow fibrocartilage contains bundles of
elastic fibres with little of no white fibrous tissue. It does not calcify or
ossify, and is not found within the musculoskeletal system.
Bone
Bone is extremely hard with a certain amount of
resilience. It is essentially an organic matrix of fibrous connective tissue
impregnated with mineral salts. The connective tissue gives the bone its
toughness and elasticity, while the mineral salts provide hardness and
rigidity, the two being skillfully blended together. It must be remembered that
the mineral component provides a ready store of calcium, which is continuously exchanged with that in body fluids,
with the rate of exchange and overall balance of these mineral ions being
influenced by several factors including hormones.
Each bone is enclosed in a dense of fibrous
tissue, the periosteum, with its form
and structure adapted to the function of support and the resistance of
mechanical stresses. Being a living tissue, bone is continually being remodeled
to meet these demands; this is particulary so during growth. The structure of
any bone cannot be satisfactorily considered in isolation, for it is dependent
upon its relationship to adjacent bones and the type of articulation between
them, as well as the attachment of muscles, tendons and ligaments to it.
The internal architecture of bone reveals
systems of trabeculae running in many
directions(picture below), arranged to resist compressive, tensile and shearing
stresses. Surrounding these trabecular systems, which tend to be found at the
ends of long bones, is a thin layer of condensed or compact bone(picture
below). The network of the trabeculae, because of its appearance, is known as cancellous or spongy bone. In the region
of the shaft of a long bone is an outer, relatively thick ring of compact bone surrounding a cavity, which
in life contains bone marrow.

Red and white blood cells are formed in red
bone marrow, which after birth is the only source of red blood cells and the
main source of white blood cells. In infants, the cavities of all of the bones
contain red marrow. However, this gradually becomes replaced by yellow fat
marrow, so that at puberty red marrow is only found in the cavities associated
with cancellous bone. With increasing age many of these regions containing red
marrow are replaced by yellow marrow. Nevertheless, red marrow tends to persist
throughout life in the vertebrae, the ribs and sternum, and the proximal ends
of the femur and humerus.
For descriptive purposes bones can be
classified according to their shape:
- Long bones are found within the limbs, and consist
of a shaft(diaphysis) and two
expanded ends(epiphyses).
- Short bones are the bones of the wrist and part of
the foot, the carpal and tarsal bones respectively.
- Flat bones are thin and tend to be curved in spite
of their classification; they include the bones of the skull vault and the
ribs. Structurally, they consist of two layers of compact bone enclosing
cancellous bone.
- Irregular bones are those which fit none of the above categories,
and include the vertebrae and many of the bones of the skull and face.
Bone development
Bone develops either directly in mesoderm by
the deposition of mineral salts, or in a previously formed cartilage model.
When the process of calcification and then ossification takes place without an
intervening cartilage model, the process is known as intramembranous ossification, with the bone being referred to as membrane bone. However, if there is an
intervening cartilage model, the process is known as endochondral ossification, with the bone being referred to as cartilage bone. This latter process is
by far the most common.
Intramembranous ossification
The site of bone formation is initially
indicated by a condensation of cells and collagen fibres accompanied by the
laying down of organic bone matrix, which becomes impregnated with mineral
salts. The formation of new bone continues in a similar manner to bone
developed in cartilage. Intramembranous ossification occurs in certain bones of
the skull, the mandible and the clavicle.
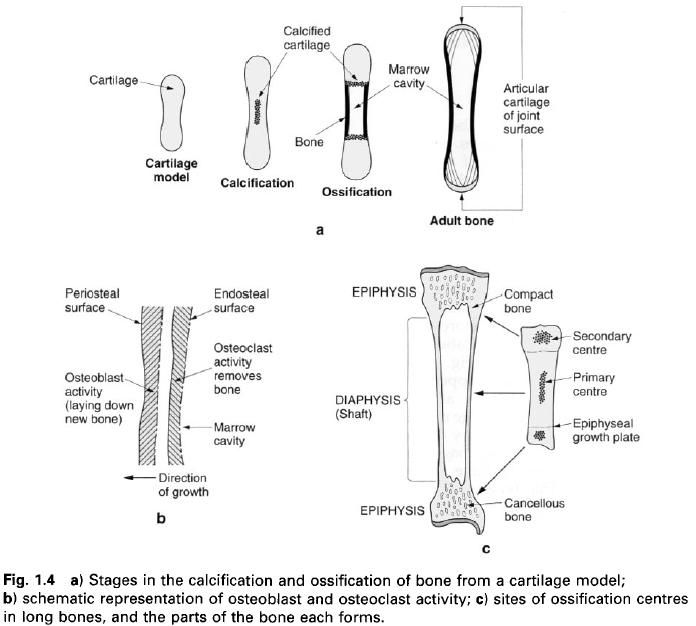
Endochondral ossification
Again the first step in the process is the
accumulation of mesodermal cells in the region where the bone is to develop. A
cartilage model of the future bone develops from these mesodermal cells(figure
a). In long bones the cartilage model grows principally at its ends, so that
the oldes part of the model is near the middle. As time progresses, the
cartilage matrix in this older region is impregnated with lime salts so that it
becomes calcified. Consequently, the cartilage cells, being cut off from their
nutrient supply, die. The greater part of the calcified cartilage is
subsequently removed and bone is formed around its few remaining
spicules(figure a). Ultimatively, the continual process of excavation of
calcified cartilage and laying down of bone leads to the complete removal of
the calcified cartilage(figure a).
The cartilage at the ends of the bone continues
to grow due to the multiplication of its cells. However the deeper layers
gradually become calcified and replaced by bone. Therefore the increase in
length of a long bone is due to active cartilage at its ends, while an increase
in width is by deposition of new bone on that already existing.
When first laid down, bone is cancellous in
appearance, having no particular pattern of organization. It is reffered to as
woven bone. In the repair of fractures, the newly formed bone also has this
woven appearance. However, in response to stresses applied to the bone by
muscles, tendons, ligaments and the forces transmitted across joints, the woven
bone gradually assumes a specific pattern in response to these stresses.
Growth and remodeling of bone
During growth there is an obvious change in the
shape of the bone. However, it should be remembered that even in the adult,
bone is being continuously remodelled, principally under the direct control of
hormones to stabilize blood calcium levels,
but also in response to long-term changes in the force patterns applied to the
bone.
Both growth and remodeling depend on the
balanced activity of two cell types, one of which removes bone tissue(osteoclasts) and the other which lays
down new bone(osteoblasts). In a
growing bone, for example, new bone is laid down around the circumference of
the shaft in order to increase its diameter. At the same time the deepest
layers of bone are being removed, thereby maintaining a reasonable thickness of
cortical bone and enlarging the marrow cavity(figure b). Should the combined
process of deposition and absorption fail to match, then either a very thick or
a very thin shaft results.
Ossification centres
The regions where bone begins to be laid down
are known as ossification centres. It is from these centres that the process of
ossification spreads. The earliest, and usually the principal, centre of
ossification in a bone is referred to as a primary
centre. Primary centres of ossification appear at different times in
different bones, but are relatively constant between individuals, and also
appear in an orderly sequence. The majority of such centres appear between the
seventh and twelfth week of intrauterine life. They are virtually all present
before birth. In long bones, the primary ossification centre appears in the
shaft of the bone(figure c).
Secondary
ossification centres appear
much later than primary ones, usually after birth, being formed in parts of the
cartilage model into which ossification from the primary centre has not spread(figure
c). All of the long bones in the body, and many others, have secondary
ossification centres. The bone formed from these centres is almost entirely
cancellous.
That part of a long bone which ossifies from
the primary centre is called the diaphysis,
while that from the secondary centre is called an epiphysis. The plate of cartilage between these two regions is
where the diaphysis continues to grow in length. Consequently, it is referred
to as the epiphyseal growth plate(figure
c). When this growth plate disappears the diaphysis and epiphysis become fused
and growth of the bone ceases.






0 коментара:
Постави коментар