Introduction
The nerves supplying the structures in the arm
are all derived from the brachial plexus, a complex of intermingling nerves
originating in the neck.
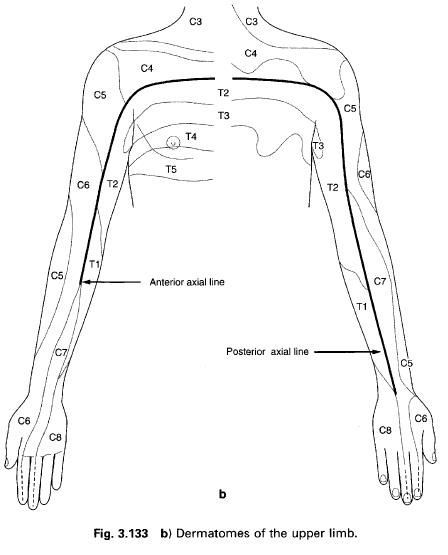
The brachial plexus is formed by the ventral rami of the lower four cervical
nerves and the first thoracic nerve to give it a root value of C5, 6, 7 and 8
and T1. Occasionally, there may be a contribution from C4 or T2 or both.
The ventral rami are found as the anterior
division of the spinal nerve, just outside the intervertebral foramen, lying
between scalenus anterior and medius. They are collectively termed the roots of
the plexus. Each spinal nerve receives an autonomic contribution, C5 and 6
receiving grey rami communicates from the middle cervical ganglion, while C7, 8,
and T1 receive them from the inferior or cervicothoracic ganglion.
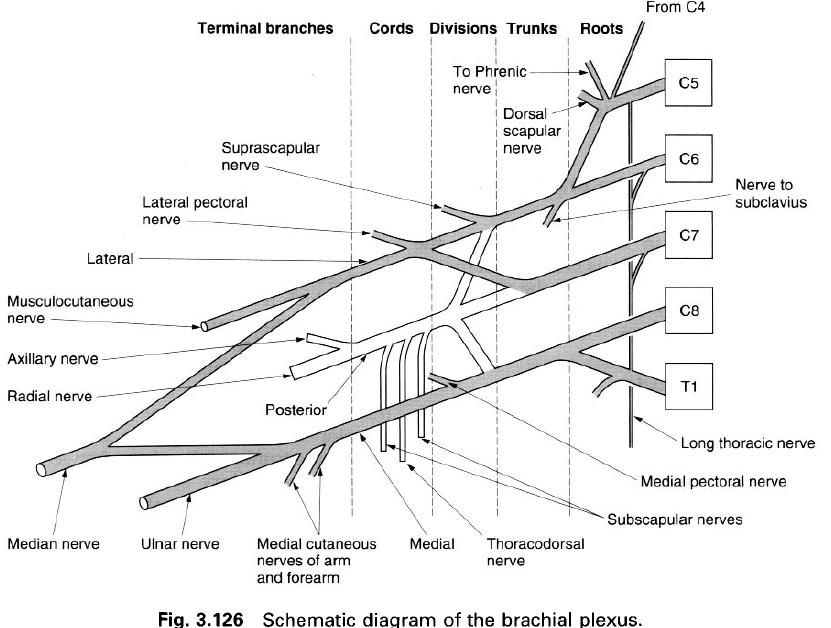
Commonly, the upper two roots(C5 and 6) unite
to form the upper trunk, the lower
two roots(C8 and T1) unite to form the lower
trunk, and the C7 root continues as the middle
trunk. These three trunks are found running between the scalene muscles and
the upper border of the clavicle in
the posterior triangle of the neck. The lower trunk may groove the upper
surface of the first rib behind the subclavian artery; the T1 root is always in
contact with the rib.
Just above the clavicle, each of the three trunks divides into an anterior and posterior division which
supply the flexor and extensor compartments of the arm respectively. The three
posterior divisions unite to form the posterior
cord, while the anterior divisions of the upper and middle trunks unite to
form the lateral cord, and the
anterior division of the lower trunk continues as the medial cord. These three cords pass downwards into the axilla,
running firstly posterolateral to the axillary artery, but then in their named
positions with respect to the second part of the axillary artery posterior to
pectoralis minor, that is medial, posterior and lateral. The cords and axillary
artery are bound together in an extension of the prevertebral fascia which
protrudes into the axilla, the axillary sheath.
Applied
anatomy
The brachial plexus itself is subject to direct
injury, consequently a knowledge of its formation is of help in determining in
exactly which parts, and at what levels, the damage has occurred. Traction
injuries occur when the roots of the plexus are torn from the spinal cord, or
when the constituent parts are partially or completely torn. In extreme cases,
the whole plexus may be disrupted to produce a completely denervated arm. If
the upper roots are completely torn, and Erb’s
paralysis affecting the musculature of the upper arm is produced; whereas
if the lower roots are completely torn, a Klumpikes’
paralysis affecting the hand and
forearm will result.
Nerves
arising from the brachial plexus and their distribution
The simplest way in which to describe the
nerves of the brachial plexus is to put them into terminological order relating
to the part of the plexus from which they originate(and to indicate their root
value).
Branches
from the roots
- Nerves to the scalene and
longus colli muscles(C5, 6, 7, 8).
- A branch to the phrenic
nerve(C5).
- The dorsal scapular
nerve(C5).
- The long thoracic
nerve(C5,6,7).
Branches
from the trunks
- The nerve to subclavius muscle(C4, 5, 6).
- Suprascapular nerve(C4, 5,
6).
There are no nerves arising from the divisions.
Branches
from the cords of the plexus
Medial
cord:
- Medial pectoral nerve(C8,
T1).
- Medial cutaneous nerve of
the forearm(C8, T1).
- Medial cutaneous nerve of
the arm(T1).
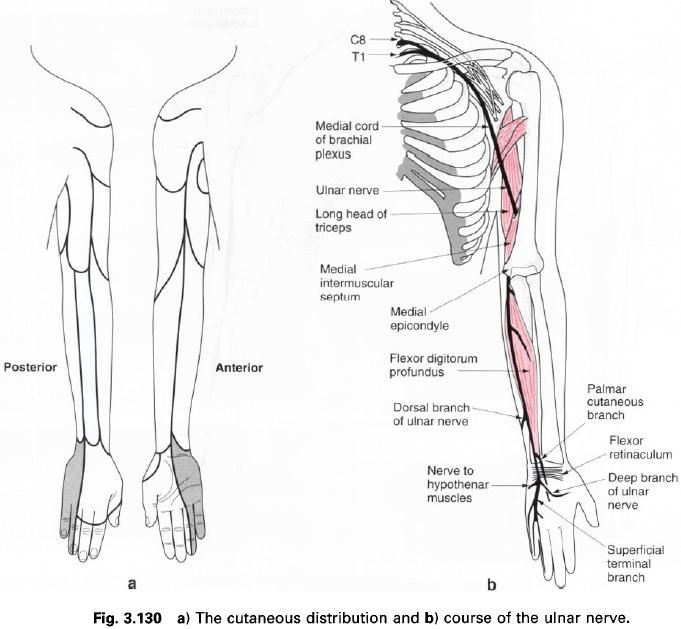
- Ulnar nerve(C7, 8, T1).
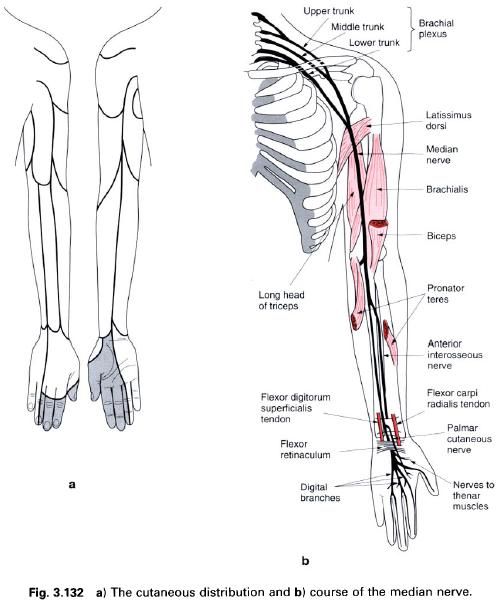
- Medial part of the median
nerve(C8, T1).
Posterior
cord:
- Upper subscapular nerve(C4,
5, 6, 7).
- Thoracodorsal nerve(C6, 7,
8).
- Lower subscapular nerve(C5,
6).
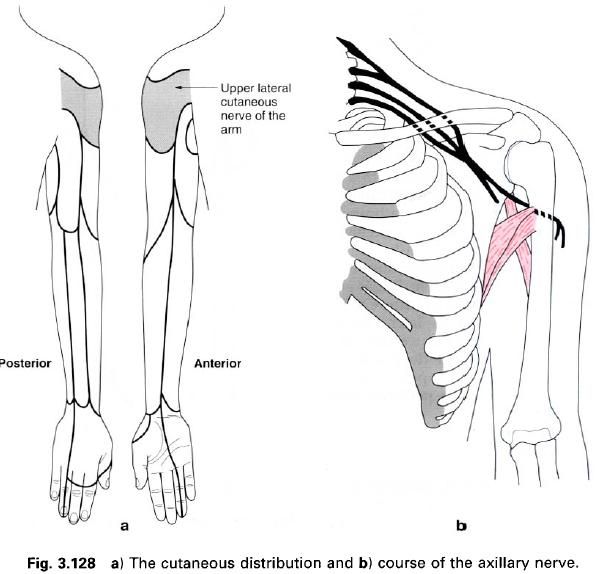
- Axillary nerve(C5, 6).
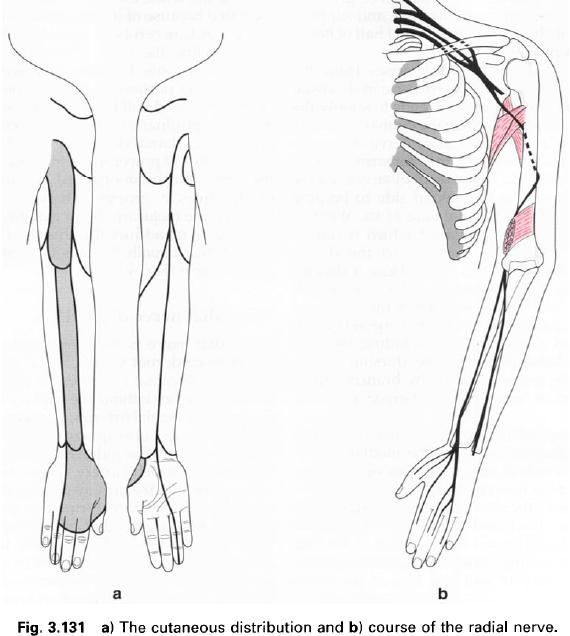
- Radial nerve(C5, C6, C7, C8,
T1).
Lateral
cord:
- Lateral pectoral nerve(C5,
6, 7).
- Musculocutaneous nerve(C5,
6, 7).
- Lateral part of the median
nerve(C5, 6, 7).
Branches
from the roots
The muscular supply to the scalene and longus
colli muscles arises by twigs from the upper surface of the anterior primary
rami as they emerge from the intervertebral foramina, directly entering the
muscles. The C5 contribution to the phrenic nerve arises as the lateral border
of scalenus anterior.
The
C5 and 6 roots of the long thoracic nerve unite after piercing scalenus medius and are joined by the C7 root on
the anterior surface of the muscle. The nerve passes behind the trunks of the
plexus between the first rib and the axillary artery to gain the
outer(axillary) surface of serratus anterior which it supplies. The upper two
digitations of the muscle are supplied by C5, the next two by C6, and the
remaining four by C7.
The
long thoracic nerve may be
damaged by direct pressure on it from above the shoulder.
The resultating paralysis of serratus anterior causes the
characteristic “winged” scapula, with
the inability to perform activities, such as abduction of the arm, where the scapula is stabilized or laterally
rotated.
Branches
from the trunks
The
nerve to subclavius(C4, 5, 6)
is a small branch from the upper trunk. It descends anterior to the subclavian
artery to supply subclavius. It may
communicate with the phrenic nerve.
The
suprascapular nerve(C4, 5, 6)
is a large branch from the upper trunk. It passes inferolaterally above and
parallel to the trunks through the suprascapular notch deep to trapezius to enter the supraspinous
fossa of the scapula. It then runs
deep to the supraspinatus muscle and
enters the infraspinous fossa via the spinoglenoid notch. The suprascapular
nerve supplies both supraspinatus and
infraspinatus, and also gives
articular filaments to the shoulder and acromioclavicular joints.
All of the above branches arise from the plexus
above the clavicle, whereas those
considered below all arise below the level of the clavicle in the axilla.
Branches
from the cords
The
lateral pectoral nerve arises
from the lateral cord of the plexus with a root value of C5, 6, 7. It crosses
anteromedially in front of the axillary artery, giving a branch to the medial
pectoral nerve before piercing the clavipectoral fascia to gain access to the
deep surface of pectoralis major
which it supplies.
The
medial pectoral nerve arises
from the medial cord with a root value C8, T1. It receives a contribution from
the lateral pectoral nerve and passes between the axillary artery and vein to gain
access to the deep surface of pectoralis minor which it supplies. It then pierces this muscle to end in pectoralis major which it also supplies.
The
upper and lower subscapular nerves both arise from the posterior cord, root values C4, 5, 6, 7 respectively.
From behind the axillary artery they descend towards the subscapular fossa
where they both supply the subscapularis muscle.
In addition, the lower subscapular nerve enters and supplies teres major.
The
thoracodorsal nerve also
arises from the posterior cord(C6, 7, 8), between the two subscapular nerves.
The nerve passes inferomedially along the posterior wall of the axilla, and the
anterolateral surface of latissimus dorsi
before entering its deep surface to supply it.
The
medial cutaneous nerve of the
arm is a small nerve arising from the medial cord(root value T1). It descends
through the axilla on the medial side of the axillary vein, and then along the
medial side of the brachial artery. It pierces the deep fascia to supply the
skin and fascia on the medial side of the proximal half of the arm, extending
onto both the anterior and posterior surfaces. It may be partly or entirely
replaced by the intercostobrachial nerve(root value T2, 3).
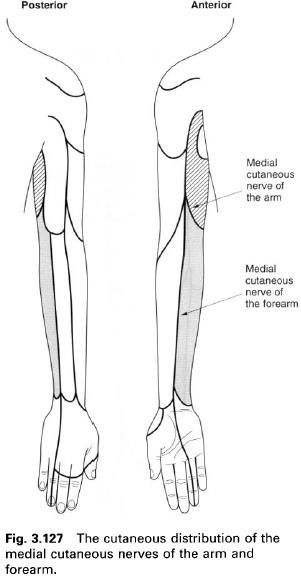
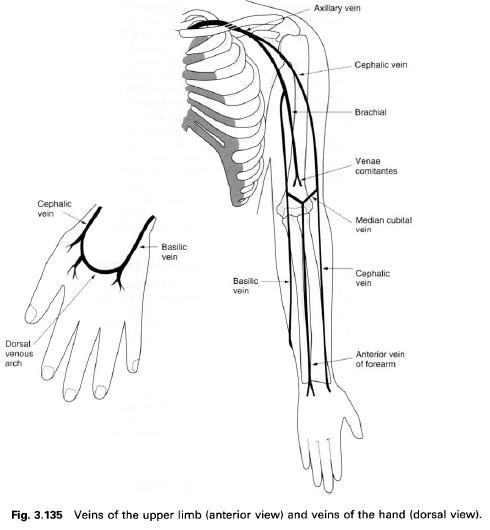
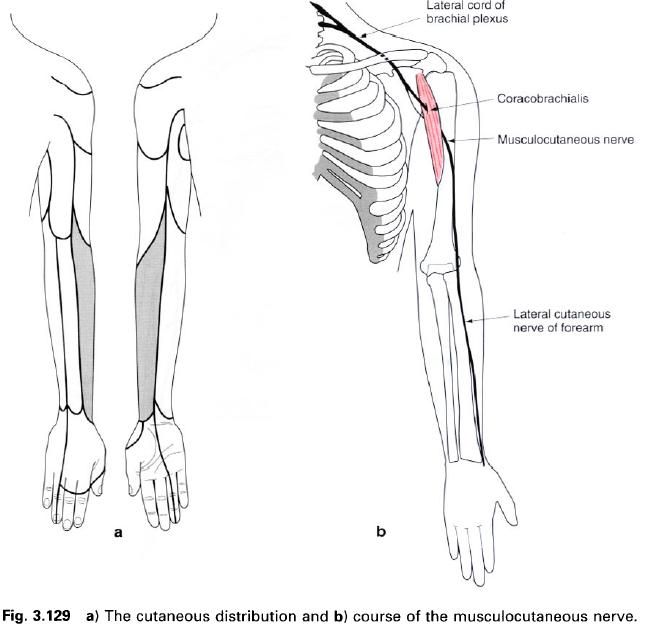
The
medial cutaneous nerve of the
forearm arises directly from the medial cord with a root value of C8, T1. It
descends on the medial side of the axillary and brachial arteries. It pierces
the deep fascia, together with basilic vein, in the middle of the arm, and
descends with it to the elbow, where it then divides into anterior and ulnar
branches. The medial cutaneous nerve of the forearm supplies the skin over the
lower part of biceps, the medial side
of the forearm as far as the wrist, and part of the medial side of the
posterior surface of the forearm.