



In general, the fingers act in one plane to
close around an object and so form a pincer action with the opposed thumb. The
size of the object being grasped will determine whether, and to what extent,
two dimensional movement at the metacarpophalangeal joints occurs.
The articulation of the second to fifth
metacarpals with the distal row of carpal bones has already been considered;
consequently, this section considers the metacarpophalangeal joints and the two
interphalangeal joints of each finger.
Metacarpophalangeal joint
The metacarpophalangeal joint of the fingers is
structurally and functionally similar to that of the thumb.
Articular
surfaces
The articular surface of the metacarpal head is
biconvex, with unequal curvatures transversely and anteroposteriorly. It is
broader anteriorly than posteriorly, with the hyaline cartilage extending
further proximally on its anterior aspect(figure a).
The base of the proximal phalanx is biconcave,
but has a smaller articular surface than the metacarpal head(figure a). The
surface area is increased by the presence of the palmar ligament attached to
the anterior margin of the articular surface.

Joint
capsule and synovial membrane
The fibrous capsule surrounding the joint is
loose, and is attached closer to the articular margins on the posterior aspects
of the bone than anteriorly. The capsule is strengthened on each side by
collateral ligaments and replaced anteriorly by the palmar ligament.
Posteriorly the extensor hood of the long extensor tendon replaces the capsule,
blending at the sides with the collateral ligaments. The posterior part of the
capsule also receives fibres from the distal slips of the palmar
aponeurosis(figure a).
The capsule is lined by synovial membrane,
which also covers all non-articular surfaces. Synovial-lined anterior and
posterior recesses of the capsule permit freedom of movement, particularly
during flexion.
Ligaments
In addition to the collateral and palmar
ligaments associated with each metacarpophalangeal joint, the heads of the
second to fifth metacarpals are united by the deep transverse metacarpal
ligaments.
The collateral
ligaments pass from the tubercle and adjacent depression on the side of the
head of the metacarpal to the palmar aspect of the side of the base of the
proximal phalanx(figure a). They are strong and tend to fan out in passing from
metacarpal to phalanx. Anteriorly they blend with the palmar ligament, while
posteriorly the extensor expansion joins them.
The palmar
ligament is a dense fibrocartilaginous plate firmly attached to the
anterior margin of the base of the proximal phalanx(figure a). Proximally it is
loosely attached to the neck of the metacarpal by the joint capsule. On each
side it receives some fibres from the collateral ligaments. The palmar ligament
acts as a mobile articular surface facilitating flexion at the joint.
The deep transverse metacarpal ligaments are a
series of short ligaments connecting the palmar ligaments of the four
metacarpophalangeal joints of the fingers(figure b). They are continuous with
the palmar interosseus fascia and blend with the fibrous flexor tendons.
Consequently, they act to bind the heads of the four medial metacarpals
together, and so limit their movement apart. (There is no ligament between the
first and second metacarpal, hence the independence and freedom of movement of
the thumb). The deep transverse metacarpal ligaments also receive fibres from
the distal slips of the palmar aponeurosis, as well as part of the extensor
expansion as it passes forwards on each side of the head of the metacarpal.
Passing behind the deep transverse metacarpal
ligaments are the tendons of both the dorsal and palmar interossei, while in
front of them pass the tendons of the lumbricals.
Blood
and nerve supply
The arterial supply to the joints is by
branches from the adjacent digital arteries, while the nerve supply is by twigs
from the median, and possibly the radial nerve for the index and middle finger,
and the ulnar nerve for the ring and little fingers. Root value of the nerve
supply is C7.
Relations
On the posterior aspect of the joint is the
expansion of the long extensor tendon(picture a below), part of which passes
around the sides of the metacarpal head blending with the deep transverse
metacarpal ligament. The tendon of the lumbrical muscle passes lateral to the
joint(a,c), anterior to the deep transverse metacarpal ligament, before
attaching to the base of the proximal phalanx and the dorsal digital expansion.
Exactly which interosseus tendons pass medial and lateral to each
metacarpophalangeal joint depends on which finger is being considered:
- for the index finger, the first dorsal interosseus is lateral and the first palmar interosseus is medial;
- for the middle finger, the second and third dorsal interossei are lateral and medial respectively;
- for the ring finger, the second palmar interosseus is lateral and the fourth dorsal interosseus is medial(figure a);
- for the little finger, the third palmar interosseus is lateral and the tendon of abductor digiti minimi is medial.
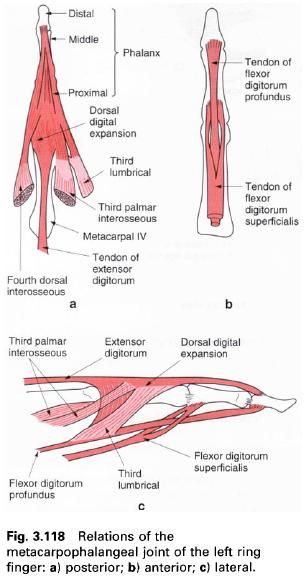
Immediately anterior to the joint is the tendon
of flexor digitorum profundus, and
anterior to that, the tendon of flexor digitorum superficialis, which at the level of the joint splits into
two(b). Flexor digiti minimi brevis
is situated on the anterolateral aspect of the joint of the little finger.
Digital branches from the dorsal and palmar
metacarpal arteries, together with digital branches from the median, ulnar and
radial nerves, depending on the finger in question, pass either side of the
metacarpophalangeal joint.
Stability
The metacarpophalangeal joint is stabilized
primarily by the long flexor and extensor tendons crossing the joint, as well
as by the lumbricals and interossei. Dislocations of the joint do occur;
however they can often be reduced by manipulation.
Movements
Active movement at the metacarpophalangeal
joint takes place about two axes, each of which is located in the metacarpal
head approximately nine-tenths of the midline length of the metacarpal from its
base. These are the movements of flexion and extension, and abduction and
adduction. To these can be added axial rotation, which occurs passively.
Flexion
and extension occur about a
transverse axis through the head of the metacarpal(figure a). The geometry of
the articular surfaces dictates that the intersection of the longitudinal axes
of the proximal phalanx and the metacarpal moves distally during flexion. In
extension the anterior surface of the metacarpal head articulates with the
palmar ligament(figure a). During flexion the ligament moves past the head,
turning upon itself to glide along the palmar surface of the shaft of the
metacarpal(figure a). As this is occurring, the capsule and its synovial lining
is being unfolded so as not to limit movement prematurely. The range of flexion
is slightly less than 90° for the index finger, but progressively increases
towards the little finger. Flexion of one joint in isolation is limited by
tension developed in the deep transverse metacarpal ligaments; flexion is
ultimately resisted by tension in the collateral ligaments. The range of active
extension is variable between subjects but may reach 50°. Passive extension may
reach as much as 90° in individuals with the lax ligaments. A study of over 400
hands gave the following total ranges of active/passive flexion and extension
for each of the fingers: index, 148° - 155°; middle, 145° - 151°, ring, 149 -
159° and little, 152° - 172°.

Flexion at the metacarpophalangeal joint is
brought about primarily by the lumbrical muscles, aided by the tendons of flexor digitorum profundus and superficialis,
as well as the interossei. In the little finger, flexor and abductor digiti minimi also contribute to the movement. Extension is achieved at all of the
metacarpophalangeal joints by extensor digitorum, with the addition of extensor indicis in the index finger and extensor digiti minimi in the little
finger.
Abduction
and adduction at the joint
occur about an anteroposterior axis through the metacarpal head; the movement
occurs away from or towards the middle finger respectively(figure a). The
movement is easier and has a greater range when the finger is extended, being
as much as 30° in each direction(figure b). Tension developed in the collateral
ligaments in flexion of the joint severely limits the side-to-side movement, so
much so that at 90° flexion the total range may be no more than 10°. The total
range of active/passive abduction and adduction movements, with the fingers in
a neutral position, has been reported as follows: index, 50°-62°; middle,
40°-53°; ring, 38°-55° and little, 57°-68°.
Abduction at the joint is brought about by the
dorsal interossei for the index, middle and ring fingers, and by abductor digiti minimi for the little
finger. At the index and middle fingers, the movement may be assisted by the
first and second lumbricals respectively via their attachment to the extensor
hood. If the joint is hyperextended, then extensor digitorum will also aid abduction. Adduction towards the middle finger is achieved
by the palmar interossei and can be assisted by the third and fourth lumbricals
for the ring and little fingers. If the joint is being flexed simultaneously,
then adduction is assisted by flexor digitorum superficialis and profundus.
Active rotation
is not possible except in little finger; however, because of the shape of the
joint surfaces and the relative laxity of the associated ligaments, a certain
degree of passive rotation can occur(figure a) having a maximum range of 60°. In
the index finger, the range of medial rotation is of the order of 45°, while
lateral rotation is negligible. Medial and lateral rotation in the remaining
fingers have approximately equal ranges of movement.








0 коментара:
Постави коментар