



The carpus is composed of eight separate bones
arranged around the capitate, but commonly described as forming two rows each
of four bones. Three of the bones in the proximal row articulate above with the
radius or articular disc at the radiocarpal joint, whilst below they articulate
with the radius or articular disc at the radiocarpal joint, whilst below they
articulate with the distal row of bones forming the midcarpal joint. The four
carpal bones of the distal row articulate with the bases of the five metacarpal
bones via the carpometacarpal joints. There are also articulations between the
adjacent carpal bones in each of the rows, the intercarpal joints.
The bones are bound together by ligaments and
so form a compact mass, which is curved to give a posterior convexity and a
pronounced anterior concavity(the carpal sulcus). This sulcus is converted into
a canal(carpal tunnel) by the flexor retinaculum.
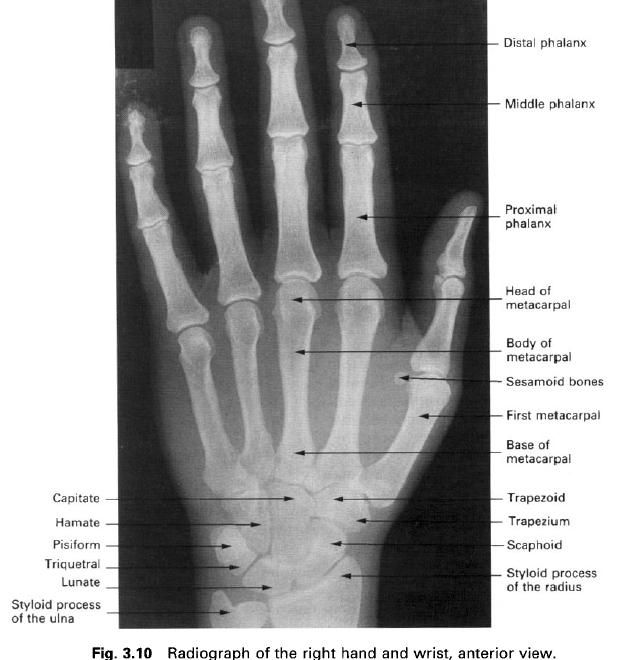
The individual carpal bones are clinically
important because they are often injured, especially the scaphoid and lunate,
and because they provide recognizable bony landmarks in the wrist region.
From lateral to medial the proximal and distal
rows are arranged as follows:
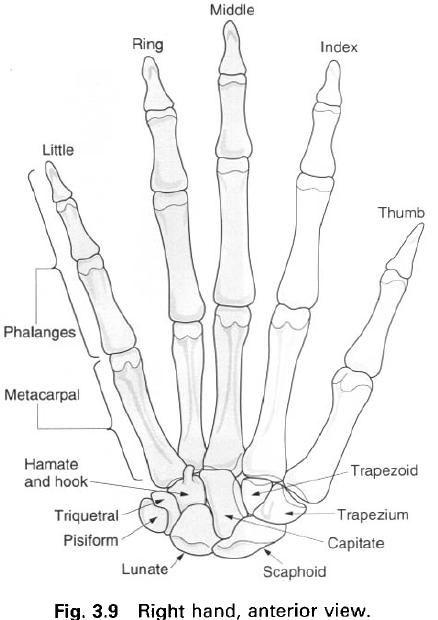
Proximal: scaphoid, lunate, triquetral,
pisiform
Distal: trapezium, trapezoid, capitate,
hamate
Proximal row
The three lateral bones to the proximal row are
so arranged as to form a convex articular surface facing proximally to fit into
the concavity formed by the radius and the articular disc. Individually, each
of the bones has a characteristic shape and its own set of articular surfaces.
Scaphoid – The scaphoid is marked anteriorly by a
prominent palpable tubercle and a narrowed waist around its centre. Articular
surfaces are present on the scaphoid: proximally for the radius, medially for
the lunate and more distally for the head of the capitate, and lateral to the
tubercle for the trapezium and trapezoid. The small, non-articular surface of
the tubercle is the only region available for the entry of blood vessels. It is
a common site of fracture.
Lunate – The lunate has a smooth convex palmar
surface which is larger than its dorsal surface. On its medial side is a square
articular surface for the triquetral, and on its lateral side a crescent –
shaped area for the scaphoid. Distally, there is a deep concavity for the head
of the capitate, while proximally the bone is convex where it articulates with
the radius and articular disc.
Triquetral – The triquetral lies in the angle between the
lunate and hamate, with which it articulates via a sinuous surface. The square
lateral articular surface is for the lunate. The triquetral is distinguished by
a circular articular surface for the pisiform. The proximal part enters the
radiocarpal joint during addiction of the hand.
Pisiform – The pisiform is a small round sesamoid bone
found in the tendon of flexor carpi ulnaris. It articulates with the palmar
surface of the triquetral. The anterior surface projects distally and laterally
forming the medial part of the carpal tunnel.
Distal row
The distal row of carpal bones presents a more
complex proximal articular surface, being flat laterally and convex medially.
Individually, the bones all have a characteristic shape.
Trapezium – The trapezium is the most irregular of the
carpal bones, with a palpable tubercle and groove medially on its anterior
surface. It has articular surfaces proximally for the scaphoid and trapezoid,
which are set at an angle to each other. Its main feature is the articular
surface for the base of the first metacarpal. This articular surface is
saddle-shaped and faces distally, laterally and slightly forwards, contributing
greatly to the mobility of the carpometacarpal joint of the thumb.
Trapezoid – The trapezoid is a small and irregular bone
which articulates with the second metacarpal. It lies in the space bounded by
the metacarpal, scaphoid, capitate and trapezium, articulating with each.
Capitate – The capitate is the largest of the carpal
bones being centrally placed with a rounded head articulating with the
concavities of the lunate and scaphoid. Medially and laterally there are
flatter articular surfaces for the hamate and trapezoid respectively. The
dorsal surface is flat, but the palmar aspect is roughened by ligamentous
attachments. The distal surface articulates mainly with the base of the third
metacarpal, but also by narrow surfaces with the bases of the second and fourth
metacarpals.
Hamate – The hamate is wedge-shaped with a large
curved palpable hook projecting from its palmar surface near the base of the
fifth metacarpal. The hook is concave on its lateral side forming part of the
carpal tunnel. The distal base of the wedge articulates with the bases of the
fourth and fifth metacarpals. The wedge passes up between the capitate and
triquetral to reach the lunate. The articular surface for the capitate is flat
and that for the triquetral is sinuous.
Overall the carpus presents a deep transverse
concavity on the palmar surface. The flexor retinaculum bridges the concavity,
attaching to the tubercles of the scaphoid and trapezium laterally, and the
pisiform and hook of hamate medially, forming the roof of the carpal tunnel.
Palpation
Starting on the medial side of the palmar
aspect of the wrist at the proximal part of the hypothenar eminence, the
pisiform can be distinquished easily with the tendon of flexor carpi ulnaris
running proximally from it. Immediately distal and slightly lateral to the
pisiform, the hook of the hamate can be palpated if sufficient pressure is
applied through the hypothenar muscles.
On the lateral side of the carpus just proximal
to the distal wrist crease, the prominent tubercle of the scaphoid can be
palpated, and immediately beyond this, the tubercle of the trapezium. The
scaphoid can be “pinched” between the palpating thumb and index finger if these
are placed on the tubercle and in the “anatomical snuff-box” at the base of the
thumb on its dorsal surface.
Ossification
Each carpal bone ossifies from a single centre,
all of which appear after birth. During the first year of life the centres for
the capitate and hamate appear. These are followed by centres for the
triquetral between 2 and 4 years, the lunate between 3 and 5 years, the
scaphoid, trapezium and trapezoid all between 4 and 6 years, and finally the
pisiform between 9 and 14 years. Ossification is not complete until between 20
and 25 years. The hook of hamate may be separate. Small additional nodules may
also be present. The shape of the individual carpal bones, and not their size,
can be used to age an individual.







0 коментара:
Постави коментар