



Supraspinatus
Deltoid
Supraspinatus
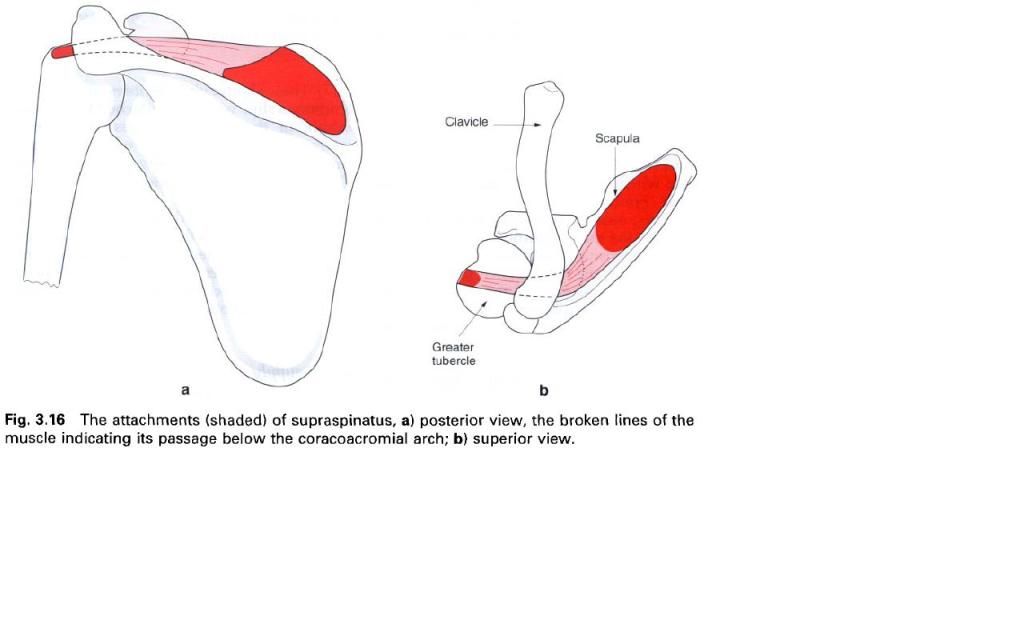
Supraspinatus arises from the medial two-thirds of the supraspinous fossa and the deep surface
of the dense fascia which covers the muscle. The muscle and the tendon which
forms within it pass laterally below trapezius,
the acromion process and the coracoacromial ligament to cross over the top of
the shoulder joint. The tendon of supraspinatus blends on its deep surface with
the capsule of the shoulder joint prior to inserting into the upper of the
three facets on the greater tubercle
of the humerus.
Nerve
supply
Supraspinatus is supplied by the suprascapular nerve, root value C5, 6, a
branch from the upper trunk of the brachial plexus. The skin over the muscle is
supplied from roots C4 and T2.
Action
Supraspinatus initiates the process of
abduction at the shoulder joint, being more important during the early part of
the movement than later when deltoid takes over. The role of supraspinatus is
probably twofold during this movement. It braces the head of the humerus firmly against the glenoid fossa
to prevent an upward shearing of the humeral head( this has been likened to a
“foot on the ladder” where a small force applied at one end will produce a
rotatory rather than a shearing movement) while at the same time producing
abduction. After the initial 20° of abduction, when the stronger deltoid takes
over, supraspinatus acts to hold the humeral head against the glenoid fossa.
Functional
activity
Supraspinatus is one of the four muscles which
form a musculotendinous cuff(or rotator cuff) around the head of the humerus. They function to keep the head
of the humerus in the glenoid fossa
during movements of the shoulder joint.
Palpation
Contraction of supraspinatus can be felt
through trapezius if the examiner’s
fingers are pressed into the medial part of the supraspinous fossa when the
subject initiates abduction at the shoulder joint. In the anatomical position,
the tendon of supraspinatus is covered by the acromion process but it can be
palpated if the subject medially rotates the shoulder with his or her hand
resting passively in the small of the back. During this manoeuvre, the greater
tubercle moves anteriorly so that the tendon can now be rolled against the bone
by a medial to lateral pressure of the examiner’s finger against the tubercle.
The tendon of supraspinatus is the most frequently damaged soft tissue in the
shoulder region and techniques, such as transverse frictions, injection and
ultrasound are often applied to this exact location. In severe cases the tendon
may be sufficiently eroded to cause its
rupture, which then affects the ease with which abduction can occur. In such
cases, or when supraspinatus is paralysed, the patient can still initiate
abduction by leaning slightly to the side so using gravity. Alternatively, the
patient may use the opposite arm to push the affected limb away from the side,
or jerk the hips to “kick” the elbow out. By each of these actions a small yet
sufficient degree of abduction occurs to enable the powerful deltoid to take
over.
Deltoid
Deltoid is a coarse, thick, triangular muscle
which gives the shoulder its rounded contour. Functionally it can be divided
into three parts, anterior, posterior and middle, of which only the middle
portion is multipennate. It has an extensive attachment to the pectoral girdle.
In front, the fibres attach to the anterior
border of the lateral third of the clavicle,
whilst behind, they come from lower lip
of the crest of the spine of the scapula. The most anterior
and posterior fibres both run obliquely, in an uninterrupted manner, to the deltoid tuberosity on the lateral
surface of the shaft of the humerus.
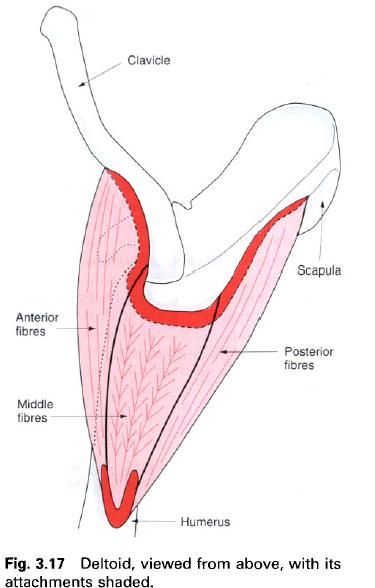
The middle muscle fibres are more complex
because of their multipennate arrangement. These shorter oblique fibres run
from four tendinous slips which are attached to the lateral margin of the acromion
process to join three intersecting tendinous slips which ultimately run to
the deltoid tuberosity of the humerus. Consequently, these shorter,
more numerous middle fibres of deltoid, working under considerable mechanical
disadvantage when active, give this part of the muscle great strength.
Deltoid is separated from the coracoacromial
arch and the upper and lateral aspects of the shoulder joint(and the tendons
lying on it) by the subacromial bursa.
Nerve
supply
Deltoid is supplied by the axillary nerve, root value C5, 6. The skin covering deltoid is
supplied by roots C4 and 5.
Action
Deltoid is the principal abductor of the arm at
the shoulder joint, the movement being produced by its middle, multipennate
fibres. However, deltoid can only produce this movement efficiently after it
has been initiated by supraspinatus.
The true plane of abduction is in line with the
blade of scapula, that is in slight
flexion, and for this the anterior and posterior fibres are active in order to
maintain the plane of abduction by acting as “guy ropes”. The tendency for
deltoid to produce an upward shearing of the head of the humerus is resisted by the muscles of the rotator cuff, that is by subscapularis anteriorly, teres minor and infraspinatus posteriorly, and supraspinatus from above.
The anterior part of deltoid is a strong flexor
and medial rotator of the humerus,
while the posterior part is a strong extensor and lateral rotator, and can help
in the transfer of the strain of heavy weights carried in the hand to the
pectoral girdle. The posterior part of deltoid is also active during adduction
of the arm, to counteract the medial rotation produced by pectoralis major and
latissimus dorsi.
Functional
activity
Deltoid is active in abduction when the middle
fibres contract concentrically, but the massive development and multipennate
nature of the muscle are probably due to the fact that many activities of the
upper limb require that it be maintained or “held” in this position for long
periods of time. Consequently, the middle fibres contract statically when
performing activities with the arms in front of the trunk; they than lower the
arm back to the side by operating in an eccentric mode.
Palpation
If the seated subject is asked to raise the arm
to 60° of abduction in the plane of the scapula,
the triangular bulk of deltoid can be felt and seen. Palpating the upper
surface of the acromion process and moving the fingers laterally from its edge,
the depressions in the muscle caused by the tendinous intersections can be felt
if anteroposterior pressure of the fingers is applied.
The anterior and posterior fibres can be made
to stand out more clearly if, in the same position as above, the subject is
asked to maintain the position against resistance first anteriorly and then
posteriorly.
Paralysis of deltoid severely affects the
functioning of the shoulder joint and therefore of the upper limb.












0 коментара:
Постави коментар