



Articular
surfaces
The articulation is between the head of the ulna and the ulnar notch on the lower
end of the radius. The joint is
closed inferiorly by an articular disc which passes between the radius and ulna thereby separating the inferior radioulnar joint from the
radiocarpal joint of the wrist.
Head
of the ulna
The head of the ulna is the slightly expanded lower end of the bone. The
crescent-shaped articular surface is situated on its anterior and lateral
aspects and is covered with hyaline cartilage, which is continuous with that on
the distal end of the ulna over a
rounded border. The distal end of the head of the ulna articulates with an intra-articular disc.

Ulnar
notch of the radius
The ulnar notch of the radius is situated between the two edges of its interosseus border,
and faces medially. It is concave anteroposteriorly and plane or slightly
concave vertically. The notch is lined by hyaline cartilage.
Articular
disc
A triangular, fibrocartilaginous articular disc
is the principal structure uniting the radius
and ulna. It attaches by its apex
to the lateral side of the root of the ulna
styloid process, and by its base to the sharp inferior edge of the ulnar notch
between the ulnar and carpal surfaces of the radius. The disc is thicker peripherally than centrally, although
it is rarely perforated.
It is an essential part of the total bearing
surface of the inferior radioulnar joint by its articulation with the distal
surface of the head of the ulna.
Inferiorly it participates in the radiocarpal joint. Perforation of its central
part would therefore lead to a communication between the inferior radioulnar
and radiocarpal joints.
Joint
capsule and synovial membrane
The relatively weak and loose fibrous capsule
is formed by transverse bands of fibres attaching to the anterior and posterior
margins of the ulnar notch of the radius,
and to the corresponding regions on the head of the ulna. The inferior margins of these bands blend with the anterior
and posterior edges of the articular disc. However, superiorly they remain
separated.
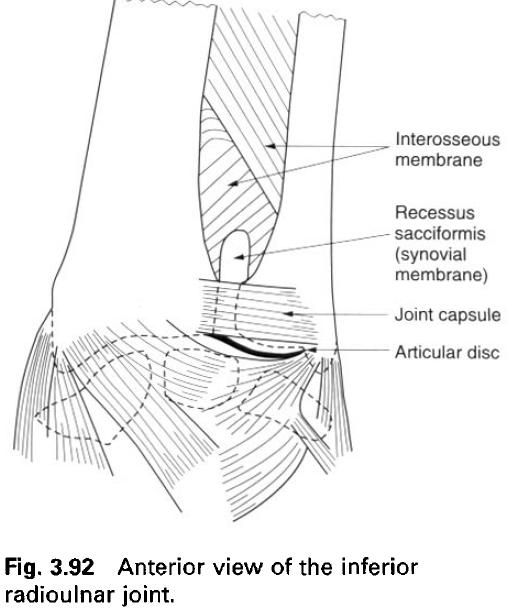
The synovial membrane is large in relation to
the size of the joint, extending upwards above the margins of the joint capsule
between the radius and ulna in front of the interosseus membrane,
to form the recessus sacciformis.
Blood and nerve supply
The arterial supply to the joint is by branches
from the anterior and posterior interosseus arteries, and from the dorsal and
palmar carpal networks, which receive branches from the radial and ulnar
arteries. Venous drainage is by similarly named vessels into the deep system of
veins. The lymphatic drainage of the joint is by vessels accompanying the
deeper blood vessels, some of which pass to nodes in the cubital fossa, but
most go directly to the lateral group of axillary nodes.
The nerve supply to the joint is by twigs from
the anterior and posterior interosseus nerves, with a root value of C7 and 8.
Relations
Passing directly behind the inferior radioulnar
joint is the tendon of extensor digiti minimi, enclosed within its synovial sheath, on its way to the little
finger. Anteriorly lies the lateral part of flexor digitorum profundus enclosed within the common flexor sheath. Proximal to
the joint pronator quadratus passes
between the radius and ulna holding them together, and thereby
protecting the joint.
Stability
Although the joint capsule is loose, to allow
for movement between the radius and ulna, the inferior radioulnar joint is
extremely stable and is rarely dislocated. The stability is due primarily to
the articular disc, but also to the interosseus membrane and pronator
quadratus.
A fall on the outstretched hand with the wrist extended frequently results in a transverse
fracture in the lower 2 or 3cm of the radius(Colles’
fracture), with the fragment being displaced posteriorly. The ulna is usually not involved except that
its styloid process may be torn off. In a Colles’ fracture the hand is displaced laterally and
dorsally. Alternatively, the fall may result in dislocation at the radiocarpal
joint, but not at the inferior radioulnar joint.
Movements
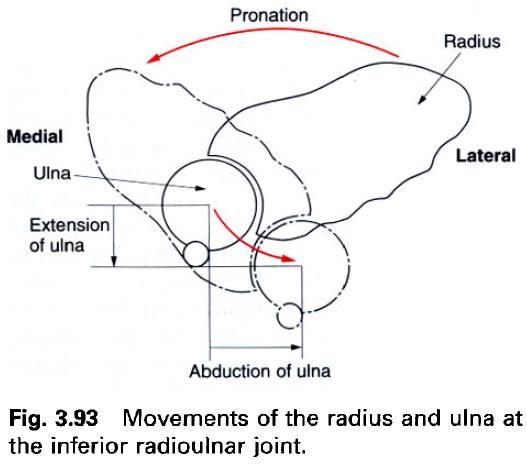
The main movement at the inferior radioulnar
joint is a rotation of the lower end of the radius
around the head of the ulna during
pronation and supination. However, because during everyday activities the axis
of pronation and supination coincides with the axis of the hand along the
middle finger, the radial rotation is accompanied by movement of the head of
the ulna. So that while the radius rotates about the ulna, the ulna is displaced with respect to the radius. The ulna
displacement observed during rotation is merely the result of two elementary
movements: slight extension and medial displacement of the ulna at the elbow. The very slight side-to-side movement possible
between the trochlea of the humerus
and the trochlear notch of the ulna
is mechahically amplified at the lower end of the ulna to become a movement of appreciable magnitude. Both the
extension and lateral displacement of the ulna
are brought about by the action of anconeus,
and therefore occur simultaneously during pronation. The arc of the movement
described by the head of the ulna
does not involve a rotation of the bone, as it remains parallel to itself
throughout, that is, the ulnar styloid process remains posteromedial.
Accessory
movements
Gripping the lower ends of the radius and ulna firmly, the head of the ulna
can be moved anteroposteriorly with respect to the radius.
Palpation
The line of the inferior radioulnar joint can
be palpated on the posterior aspect of the wrist, running vertically between
the two bones.
Interosseus membrane
The interosseus membrane stretching between the
interosseus borders of the radius and
ulna is a strong, fibrous sheet whose
fibres predominantly pass obliquely downwards and medially from the radius to the ulna. Being deficient superiorly, it has a free oblique border
which is attached 2 to 3cm below the radial tuberosity and passes to a slightly
lower level on the ulna. Inferiorly
the membrane is continuous with the fascia on the posterior surface of pronator quadratus, attaching to the
posterior of the two lines into which the radial interosseus border divides. An
opening in the lower part of the membrane enables the anterior interosseus
vessels to pass into the posterior compartment of the forearm. On the posterior
part of the membrane there are a small number of fibrous bands which pass
obliquely downwards and laterally. During pronation and supination, tension in
the membrane varies, being greatest in the midprone position.

The oblique direction of the fibres of the
interosseus membrane serves to transmit forces from the radius to the ulna. The radius is the forearm bone articulating
at the radiocarpal joint, receiving impacts and forces from the scaphoid and
lunate. At the elbow, however, it has a rather ineffective articulation with
the humerus, whereas the ulna has a large and firm articulation.
The membrane serves to transmit forces carried from the hand up through the radius to the ulna and thence to the elbow joint and humerus.
As well as providing a firm connection between
the radius and ulna the interosseus membrane separates and increases the area of
attachment of the deep muscle of the anterior and posterior compartments of the
forearm.
Above the upper free border of the interosseus
membrane the oblique cord passes upwards and medially from the radius to the ulna. It is a slender, flattened fibrous band, which is said to
represent a degenerated part of flexor pollicis longus or supinator,
attached just below the radial tuberosity and to the lateral border of the
ulnar tuberosity. In the gap between the oblique cord and the interosseus
membrane, the posterior interosseus vessels pass to and form the posterior
compartment of the forearm.
Pronation and supination
In the supine position, the bones of the
forearm lie parallel to one another(a); in the anatomical position the palm of
the hand therefore faces forwards. In
the prone position, the bones of the forearm cross one another(a), with the radius lying anterior to the ulna; with reference to the anatomical
position the palm faces backwards. The movement which causes crossing of the radius and ulna is called pronation, while that causing them to become
parallel is called supination. The movements between the radius and ulna occur at
the superior and inferior radioulnar joints.
The muscles producing pronation are pronator teres and pronator quadratus, with pronator teres being the more powerful of the two. Flexor carpi radialis, because of its oblique course, can and does
assist in pronation. Supination is produced by supinator and biceps brachii,
of which biceps is by far the
stronger. However, when the elbow is fully extended biceps is unable to act as a supinator because its tendon runs
almost parallel to the shaft of the radius,
and so cannot produce radial rotation. Of the two movements supination is the
more powerful. Because the majority of the population are right-handed, screws
have a right-hand thread. If you are trying to move a particularly stubborn
screw from a cabinet or door frame, ask a left-handed friend to do it! Both
pronation and supination are most powerful when the elbow is flexed to 90°.

The axis of pronation and supination can vary
depending about which finger the movement is occurring. It always passes
through the centre of the head of the radius,
but at the level of the wrist it can pass through any point between the ulnar
and radial styloid processes. Nevertheless, it will tend to lie in the medial
half of this region in most instances. Therefore, to state that the axis runs
between the centre of the radial head and the base of the ulnar styloid process
is not strictly correct. When rotation occurs about a more laterally placed
centre at the wrist, ulnar movement at the trochlea is insufficient.
Consequently, with the elbow flexed the movement is supplemented by rotation of
the humerus.
The forearm can be pronated through almost 180°,
without medial rotation of the humerus(b).
The constraint to further movement comes predominantly from the passive
resistance of the opposing muscles, and not from ligamentous ties. However, if
the humerus is allowed to rotate then
it becomes possible to turn the hand through almost 360°.
Pronation and supination are frequently used
movements in many activities. Consequently loss of the ability to pronate and
supinate can be a marked disability. When these movements are lost it is less
disabling if the forearm is fixed in a midprone position, so that the palm
faces medially.






0 коментара:
Постави коментар