



Blood and nerve supply
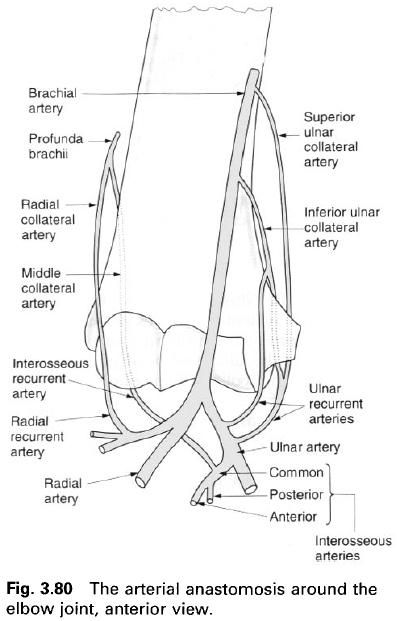
The arterial blood supply to the joint is
derived from an extensive anastomosis around the elbow involving the brachial
artery and its terminal branches. Descending from above are the superior and
inferior ulnar collateral branches of the brachial artery, and the radial and
middle collateral branches of the profunda brachii artery. These vessels
anastomose on the surface of the joint capsule with one another, and with the
anterior and posterior recurrent branches of the ulnar artery, the radial
recurrent branch of the radial artery and the interosseus recurrent branch of
the common interosseus artery.
Venous drainage, by vessels accompanying the
above arteries, is into the radial, ulnar and brachial veins. Lymphatic
drainage of the elbow joint is predominantly to the deep cubital nodes at the
bifurcation of the brachial artery, the efferents of which pass to the lateral
group of nodes in the axilla. Some of the lymphatics from the joint may pass to
small nodules situated along the interosseus, ulnar, radial or brachial
arteries and thence to the lateral axillary group.
The nerve supply to the joint is by twigs
derived anteriorly from the musculocutaneous, median and radial nerves, and
posteriorly from the ulnar nerve and radial nerve by its branch to anconeus.
The root value of these nerves is C5, 6, 7 and 8.
Palpation
Palpation of the joint line anteriorly is not
possible because of the muscles crossing the joint and its deepness within the
cubital fossa. Nevertheless, it can be approximated by drawing a line joining
the points 1cm below the lateral epicondyle and 2cm below the medial
epicondyle. Posteriorly the gap between the head of the radius and the capitulum can be palpated in the large dimple
present at the back of the extended elbow.
Relations
Posteriorly the olecranon is subcutaneous and
can be readily palpated. Either side of the olecranon the medial and lateral
epicondyles form easily recognizable bony land marks. Anteriorly lies brachialis forming the majority of the
floor of the cubital fossa, a hollow in front of the elbow through which pass
many of the vessels and nerves entering or leaving the forearm.
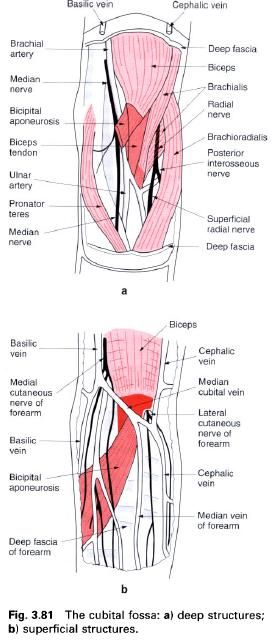
The cubital fossa is a triangular space bounded
above by an imaginary line between the medial and lateral epicondyles, and at
the sides by the converging medial borders of brachioradialis laterally and pronator teres medially(a). The floor of this region is formed mainly by brachialis with supinator inferolaterally(a). It is roofed over by the deep fascia
of the forearm, reinforced medially by the bicipital aponeurosis passing from
the tendon of biceps downwards and
medially to the deep fascia of the forearm(b). The deep fascia separates the
superficial veins and nerves from the deeper more important structures(b).
This region is of considerable importance
because the large superficial veins are frequently used for venepuncture, while
the deeper brachial artery is used for determining blood pressure. The main
superficial veins are the cephalic laterally, the basilica medially and the
median cubital passing obliquely upwards and medially between them(b). It is
not unusual for the median cubital vein to lie towards the lateral side of the
fossa, or to be joined by the median vein of the forearm. Occasionally, the
median cubital vein is absent and the median vein of the forearm divides into
lateral and medial branches to join with the cephalic and basilic veins
respectively. Lateral to the cephalic vein runs the lateral cutaneous nerve of
the forearm, the terminal branch of the musculocutaneous nerve. Crossing the
median cubital vein and running with the basilica vein and its tributaries are
branches of the medial cutaneous nerve of the forearm(b).
Lying within the cubital fossa deep to the deep
fascia are several structures passing into the forearm. The most medial of
these is the median nerve as it passes downwards through the fossa to emerge
between the two heads of pronator teres
and thus enter the forearm(a). While in the fossa it gives off a branch to pronator teres, and the anterior
interosseus branch as it passes through pronator teres. Lateral to the median nerve is the brachial artery, which bifurcates
into the ulnar and radial arteries at the neck of the radius in the lower part of the fossa(a). The ulnar artery passes
inferomedially deep to pronator teres,
giving off recurrent branches to the elbow joint and the common interosseus
artery. The radial artery passes inferolaterally on the tendon of biceps brachii deep to brachioradialis, giving off its
recurrent branch to the elbow joint. Running through the central region of the
fossa, lateral to both the brachial artery and the median nerve is the tendon
of biceps brachii towards its
insertion on the radial tuberosity(a). As it passes through the fossa the
tendon twists on itself so that its anterior surface faces laterally. The most
lateral structure passing through the fossa is the radial nerve. In the upper
part of the fossa it lies submerged between brachialis and brachioradialis supplying both
muscles, and then divides into its terminal branches, the superficial radial
and posterior interosseous(deep radial) nerves. The superficial branch
continues downwards into the forearm under cover of brachioradialis. The posterior interosseus nerve passes backwards
around the lateral side of the radius to
enter the forearm between the two heads of supinator.
The ulnar nerve, passing behind the medial
epicondyle of the humerus on the
intermediate part of the ulnar collateral ligament, lies posteromedial to the
elbow joint. It therefore does not pass through the cubital fossa.
Stability
Stability of the elbow joint is by virtue of
the shape of the articular surfaces of the trochlea and capitulum of the humerus, and the trochlear notch of the ulna and head of the radius. Without strong collateral
ligaments and the muscular cuff of triceps,
biceps, brachialis, brachioradialis, and the common tendons of the
superficial flexors and extensors arising from the medial and lateral
epicondyles of the humerus, the elbow
joint cannot be considered as an inherently stable joint. The bony surfaces are
in closest contact when the forearm is flexed to 90° in a position of mid
pronation – supination. This, therefore, is the position naturally assumed when
fine manipulation of the hand and
fingers is required, as for example when writing.
In spite of ligaments and muscles crossing the
joint, dislocations of the elbow can and do occur. In the child, because the
head of the radius is small relative
to the annular ligament, it is commonly dislocated by traction forces applied
to the forearm and hand. In older
people, a fall on the hand with the
forearm extended may tear the annular ligament with a consequent anterior
displacement of the head of the radius(a).
The head of the radius may also be
dislocated by extreme pronation, by tearing the annular ligament. In either
case it can be palpated in the cubital fossa.
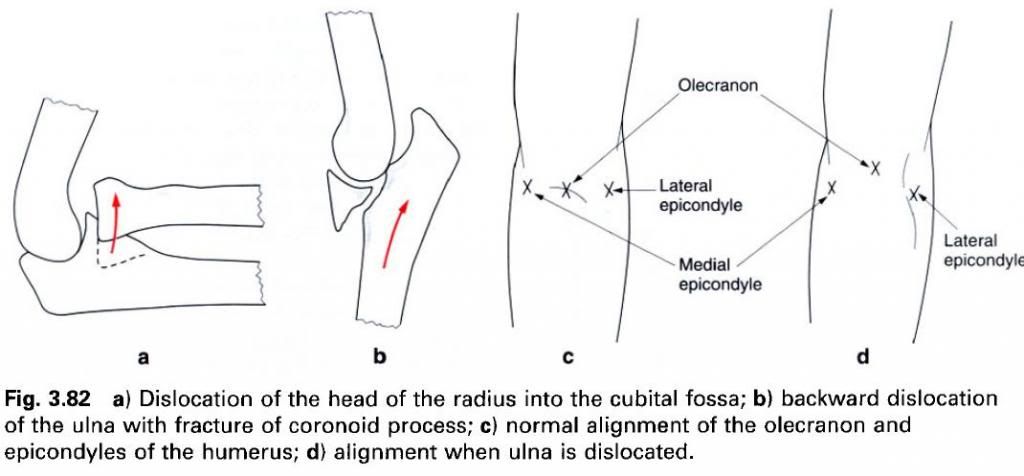
The majority of elbow dislocations involve a
backward movement of the ulna,
through the relatively weak posterior capsule, and is often associated with a
fracture of the coronoid process(b). Both radius
and ulna may be displaced together due to their connections at the superior
radioulnar joint. This backward at the superior radioulnar joint. This backward
displacement can lead to pressure on the brachial artery which may go into
spasm and reduce and blood supply to the forearm and hand. Pressure on the brachial artery can also arise in
supracondylar fractures as the lower fragment moves forwards. Either of these events
can also lead to injury of the median nerve with a consequent loss of pronation
and reduced use of the hand. Both
dislocations and supracondylar fractures result in considerable swelling in the
region of the elbow. The alignment of the epicondyles of the humerus and the olecranon can be used to
determine the nature of the trauma in an individual with a swollen elbow. The
alignment remains unchanged in supracondylar fractures(c), while in
dislocations it is changed(d). When an apparently dislocated joint cannot be
reduced, fracture of the olecranon must be considered, particularly if the
joint is extremely unstable.
A forceful abduction applied to the forearm may
be sufficient to rupture that ulnar collateral ligament, or more commonly
result in avulsion of the medial epicondyle. The ulnar nerve is especially
liable to damage at the time of the injury. If the fracture does not unite or
the ligament heal, the forearm tends to become more and more abducted with a
consequent stretching of the ulnar nerve, leading to sensory disturbances and
muscle weakness or paralysis.











0 коментара:
Постави коментар