



Introduction
The elbow joint is the intermediate joint of
the upper limb, being between the arm and the forearm. It can be considered to
be subservient to the hand in the
sense that it enables the hand and
fingers to be properly placed in space. The elbow joint is responsible for
shortening and lengthening the upper limb; the ability to carry food to the
mouth is due to flexion at the elbow. If situations arise in which the hand and forearm are not able to move,
then the arm and trunk can move towards the hand.
The elbow joint is a synovial joint of the
hinge variety, and shares, with the superior radioulnar joint, the same joint
capsule. The superior radioulnar joint has no function at the elbow and plays
no part in its movements. The elbow joint shows the fundamental characteristics
of all hinge joints. The articular surfaces are reciprocally shaped; it has
strong collateral ligaments with the forearm muscles grouped at the sides of
the joint where they do not interfere with movement.

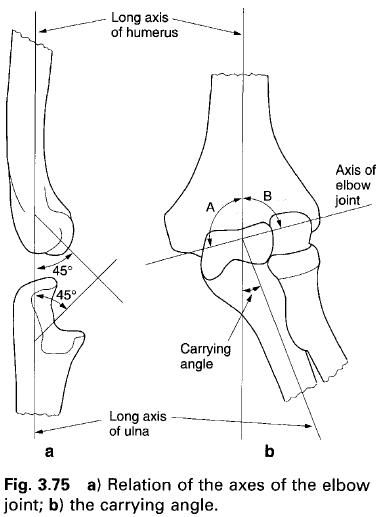
When viewed laterally, the distal end of the humerus bulges anteriorly and inferiorly
at an angle of 45° so that the trochlea lies anterior to the axis of the
shaft(a). In a similar way the trochlear notch of the ulna projects anteriorly and superiorly at an angle of 45°, and so
lies anterior to the axis of the shaft of the ulna(a). The projection of these two articular surfaces facilitates
and promotes a large range of flexion at the elbow. It delays contact between
the two bones, in addition to which there is still a space between them to
accommodate the musculature until the bones are almost parallel. Without these
two features, particularly the first, flexion beyond 90° would be severely
limited.
In spite of the anterior projections of the humerus and ulna the long axes of the two bones coincide when viewed laterally.
However, when seen from the front, the ulnar axis deviates laterally from that
of the humerus(b). This deviation is
referred to as the carrying angle, and is said to be approximately 10° to 15°
in men and 20° to 25° in women. Normally, the transverse axis of the elbow
joint bisects this angle so that when the elbow is acutely flexed the forearm
overlies the arm, and tha hand covers
the shoulder joint. If, however, the bisected parts of the carrying angle are
not equal then the hand will be
lateral to the shoulder( A < B, figure b) or medial to the shoulder(A >
B, figure b) on acute flexion at the joint.
The transverse axis of the elbow joint runs
from inferior posteromedially to superior anterolaterally passing approximately
through the middle of the trochlea. Because of this slight obliquity there has
been some debate as to whether the joint exhibits a pure hinge movement,
especially as this axis also oscillates slightly. However, for practical
purposes it can be considered as a pure hinge joint.
Articular surfaces
Three bones are involved in the articulation at
the elbow joint; these are the distal end of the humerus, and the proximal ends of the radius and ulna. The
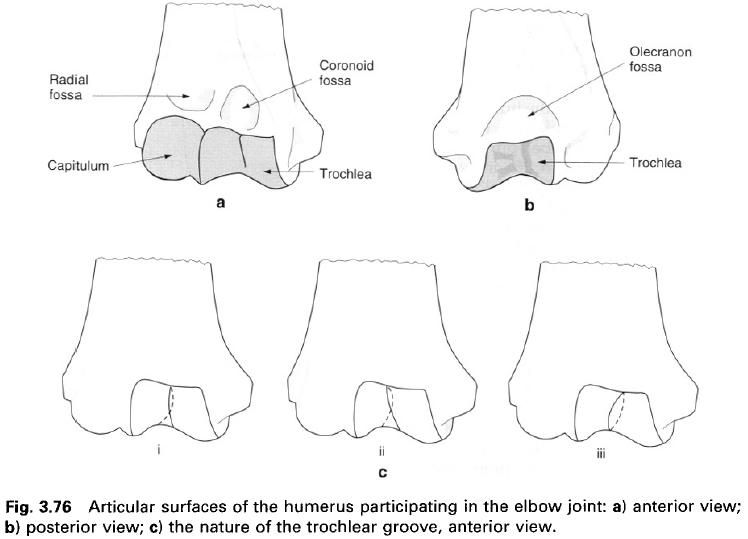
distal end of the humerus shows two
joined articular regions: the grooved trochlea medially and the rounded
capitulum laterally, being separated by a groove of variable depth(a). The
whole of this composite surface is covered by a continuous layer of hyaline
cartilage. The trochlea articulates with the trochlear notch of the ulna, while the capitulum articulates
with the cupped head of the radius.
Both of these latter surfaces are also covered with hyaline cartilage.
Trochlea
of the humerus
The pulley-shaped trochlea with its groove
presents a concave surface in the frontal plane and is convex sagitally. It
forms almost a complete circle, being separated by a thin wall of bone, which
itself may be perforated, so that 320° to 330° of the surface is cartilage
covered(a, b). The medial free border of the trochlea is not circular but
describes part of a helix with a slant directed radially. The groove of the
trochlea is limited medially by a sharp and prominent ridge and laterally by a
lower and blunter ridge which blends with the articular surface of the
capitulum(a). The tilt of the trochlea partly accounts for the carrying angle
of the elbow.
Although the groove of the trochlea appears to
lie in the sagittal plane it does in fact run obliquely. This obliquity shows
individual variation; however the most common form is with the anterior part of
the groove being vertical and the posterior part running obliquely distally and
laterally. As a whole the groove runs in a spiral around the axis of the
bone(c). Occasionally, the groove runs obliquely proximally and laterally at
the front and distally and laterally at the back, and so as a whole forms a
true spiral around the axis of the bone(c). Finally, and rarely, the groove may
run obliquely proximally and medially anteriorly, and distally and laterally
posteriorly, so that as a whole it forms a circle(c). The functional
significance of these variations in the angulation of the trochlea is minimal.
The only observable differences are in the degree of the carrying angle and the
relative positions of the arm and forearm in acute flexion at the elbow.
Immediately above the trochlea anteriorly is
the concave coronoid fossa(a), which receives the coronoid process of the ulna during flexion. Posteriorly, in a
similar position, is the olecranon fossa which receives the olecranon process
during extension(b). If these two fossae are particularly deep the intervening
thin plate of bone may be perforated allowing them to communicate with each
other.
Capitulum
The capitulum is not a complete sphere but a
hemisphere on the anterior and inferior surface of the humerus(a). It does not extend posteriorly like the trochlea. Although
described as hemispherical, its radius of curvature is not constant, increasing
slightly from proximally to distally. The cartilage covering the capitulum is
thickest in its central region, and may be as much as 5mm thick. The medial
border of the capitulum is truncated forming the capitulotrochlear groove.
Above the capitulum anteriorly is the radial fossa which receives the rim of
the head of the radius during
flexion(a).
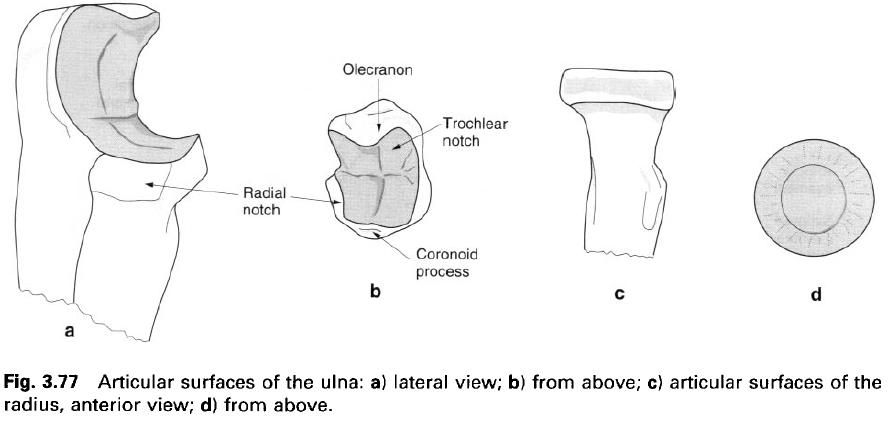
Trochlear
notch of the ulna
The proximal end of the ulna has the deep trochlear notch which articulates with the
trochlea(a, b). It has a rounded, curved longitudinal ridge extending from the
tip of the olecranon process superiorly to the tip of the coronoid process
inferiorly. The ridge snugly fits the groove of the trochlea, on either side of
which is a concave surface for the lips of the trochlea. The cartilage of the
trochlear notch is interrupted by a transverse line across its deepest part,
providing two separate surfaces, one on the olecranon and the other on the
coronoid process.
The obliquity of the shaft of the ulna to the ridge accounts for the
majority of the carrying angle.
Head
of the radius
The superior surface of the head of the radius is concave for articulation with
the capitulum, with the raised margin articulating with the capitulotrochlear
groove(c,d). The cartilage of this surface is continuous with that around the
sides of the head: it is thickest in the middle of concavity.
Because of the articulations between the radius and ulna, their proximal surfaces may be considered as constituting a
single articular surface. However, because of the movements between these two
bones, they do not maintain the same relative positions with respect to the humerus, nor does the radius always
maintain contact with the humerus.
As indicated previously, the articular surface
of the trochlea has an angular value of 330°, while that of the capitulum is
180°(a, b). The angular values of the articular surfaces of the ulna and radius are much smaller, leaving a large portion of the humeral
surfaces exposed at all positions of the joint. The angular value of the
trochlear notch is 190°, while that of the head of the radius is only 40°. The difference in angular values between
corresponding parts of the elbow is therefore 140°, a value very close to the range of flexion –
extension possible at the joint.
Joint capsule and synovial membrane
A fibrous capsule completely encloses the elbow
joint and also surrounds the superior radioulnar joint. It has no openings in
it, but slight pouching of the synovial membrane may occur beneath the edge of
the capsule in one or two areas.
Anteriorly the capsule arises from the medial
epicondyle away from the articular surface of the trochlea. It arches upwards
and laterally attaching to the margins of the coronoid and radial fossae, and
to the articular margin of the capitulum as it reaches the lateral epicondyle.
Posteriorly, the capsule follows the lateral margins of the capitulum and
arches upwards around the olecranon fossa, returning to the medial epicondyle
some distance from the edge of the trochlear surface.
Distally the capsule attaches to the margins of
the trochlear notch around the olecranon and coronoid processes. As the capsule
reaches the region of the radial notch it passes on to and attaches to the
annular ligament of the radius.
Medially and laterally it blends with the collateral ligaments of the joint. It
should be remembered that the joint capsule has no direct attachment to the radius. If this were the case, then the
movements possible between the radius
and ulna would be severely limited.
Because it blends with the collateral ligaments
at the sides, the capsule is strengthened in these regions; however, it is
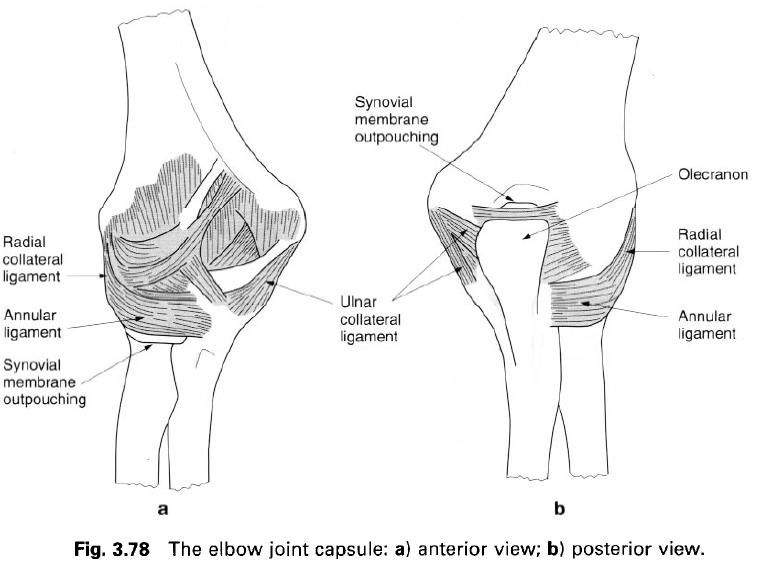
relatively weak in front and behind. Anteriorly the capsule consists mainly of
longitudinal fibres running from above the coronoid and radial fossae on the humerus to the anterior border of the
coronoid process and front of the annular ligament(a). Among these longitudinal
fibres are some bundles which run obliquely and transversely(a). Consequently,
this part of the capsule is thicker in its middle region than at the sides; a
feature which has led to it being referred to as the capsular ligament. Some of
the deep fibres of brachialis insert
into the front of the capsule as the muscle passes anteriorly across the joint.
This attachment serves to pull the capsule and underlying synovial membrane upwards
when the joint is flexed, thereby preventing them becoming trapped between the
two moving bones.
The posterior part of the capsule is thin and
membranous, being composed mainly of transverse fibres extending loosely
between the margins of the olecranon and the edges of the olecranon fossa. A
few fibres stretch across the fossa as a transverse band with a free upper
border, which does not reach as high as the upper margin of the fossa, without
attaching to the olecranon(b). Posteriorly the capsule also passes laterally
from the lateral epicondyle to the posterior border of the radial notch and the
posterior part of the annular ligament. The weakest part of the capsule
posteriorly is in the midline of the joint. However, here it is attached to the
tendon of triceps which supports it,
and performs a similar function to the deep part of brachialis in extension at the joint.
Synovial membrane
The synovial membrane of the joint is extensive
attaching to the articular margins of the humerus
and ulna. It lines the joint capsule
and is reflected onto the humerus to
cover the coronoid and radial fossae anteriorly and the olecranon fossa
posteriorly. Distally it is prolonged onto the upper part of the deep surface
of the annular ligament. The membrane is continued into the superior radioulnar
articulation covering the lower part of the annular ligament, and is then
reflected onto the neck of the radius.
Below the lower border of the annular ligament, the membrane emerges as a
redundant fold to give freedom of movement to the head of the radius(a). This downward reflection is
supported by a few loose fibres which pass from the lower border of the annular
ligament to the neck of the radius.
The quadrate ligament supports the synovial membrane as it passes from the
medial side of the neck of the radius
to the lower border of the radial notch, so preventing its herniation between
the anterior and posterior free edges of the annular ligament.
Various synovial folds project onto the
processes of the joint between the edges of the articular surfaces. An
especially constant fold is one which forms almost a complete ring overlying
the periphery of the head of the radius,
projecting onto the crevice between it and the capitulum. Slight pouching of
the synovial membrane may occur below the lower borders of the annular ligament
and the transverse band of the ulnar collateral ligament; and above the
transverse capsular fibres across the upper part of the olecranon fossa(b).
Well – marked extrasynovial fat pads lie
adjacent to the articular fossae. In extension of the joint, they fill the
radial and coronoid fossae, and in flexion the olecranon fossa. They are
displaced when the appropriate parts of the ulna
or radius occupy the fossae.
Ligaments
The collateral ligaments are strong triangular
bands which blend with the sides of the joint capsule. They are placed so that
they lie across the axis of movement in all positions of the joint.
Consequently, they are relatively tense in all positions of flexion and
extension, and impose strict limitations on abduction and adduction movements
and axial rotation.
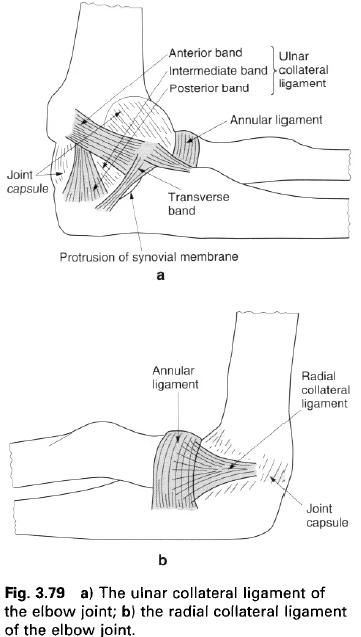
Ulnar
collateral ligament
The ulnar collateral ligament fans out from the
medial epicondyle and has thick anterior and posterior bands united by a
thinner intermediate portion(a). The anterior band passes from the front of the
medial epicondyle to the medial edge of the coronoid process. It is intimately
associated with the common tendon of the superficial forearm flexor muscles,
giving rise to some of the fibres of flexor digitorum superficialis. The posterior band runs from the back of the
medial epicondyle to the medial edge of the olecranon. The apex of the thinner
intermediate part of the ligament is attached to the undersurface of the medial
epicondyle, while its base is attached to the transverse band stretched between
the attachments of the anterior and posterior bands to the coronoid process and
olecranon(a). The synovial membrane tends to protrude below the free edge of
the transverse ligament during movement at the joint. The intermediate grooved
part of the ligament is crossed by the ulnar nerve as it passes behind the
medial epicondyle to gain access to the forearm.
Radial
collateral ligament
The radial collateral ligament is a strong,
triangular band attaching above to a depression on the anteroinferior aspect of
the lateral epicondyle deep to the overlying common extensor tendon(b). Below,
the ligament blends with the annular ligament of the radius, the slightly thicker anterior and posterior margins passing
forwards and backwards to attach to the margins of the radial notch on the ulna(b). The ligament is less distinct
than the ulnar collateral.












0 коментара:
Постави коментар