



PART I
PART II
PART II
Movements
The architecture of the shoulder joint gives it
a greater range of movement than at any other joint within the body. Its ball
and socket shape means that movement can take place around an infinite number
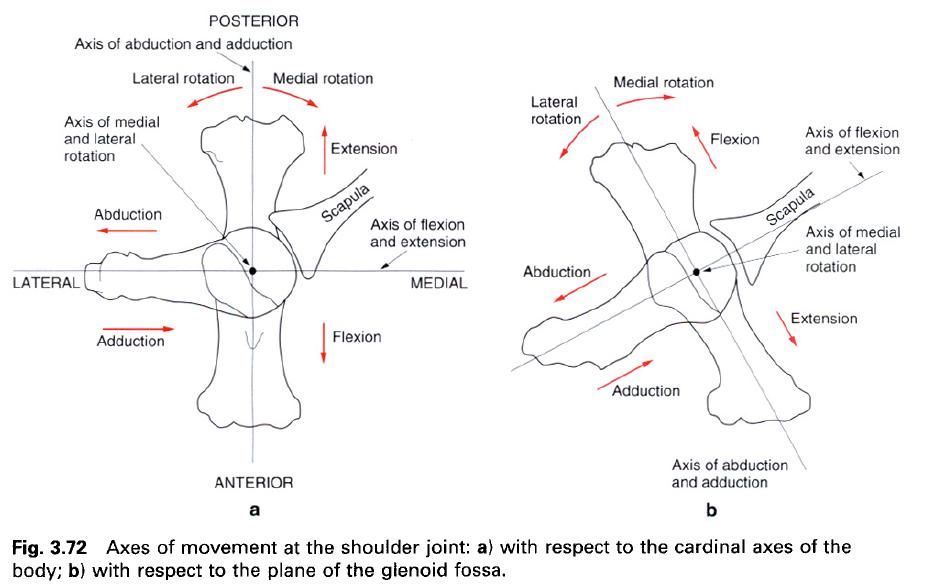
of axes intersecting at the centre of the head of the humerus. For descriptive purposes, the movements of which the
shoulder joint is capable are flexion and extension, abduction and adduction,
and medial and lateral rotation. However, the axes about which they occur have
to be carefully defined as the plane of the glenoid fossa does not coincide
with one of the cardinal planes of the body, but is inclined approximately 45°
to both of the frontal and sagittal planes. It is thus possible to define two
sets of axes about which movements occur, one with respect to the cardinal
planes of the body(a) and the other with respect to the plane of the glenoid
fossa(b). If the cardinal planes are used, flexion and extension occur about a
transverse axis, abduction and adduction occur about an anteroposterior axis,
and medial and lateral rotation occur about the longitudinal axis of the humerus, passing between the centre of
the head and the centre of the capitulum(a). If, however, the plane of the scapula is used to determine these
various axes, then flexion and extension take place about an axis perpendicular
to the plane of the fossa, abduction and adduction about an axis parallel to the plane of the fossa, with medial and
lateral rotation occurring about the same axis as previously(b). While the
presentation of these two sets of axes may seem initially confusing, the
importance of those related to the plane of the glenoid fossa is that in the
treatment of certain injuries of the shoulder, the position of the joint which
will cause the greatest relief will be when the capsule is not put under
tension, that is when the joint is abducted to 90° in the plane of the glenoid
fossa.
Irrespective of the orientation of these axes,
the incongruity of the joint surfaces means that all movements, except axial
rotation, are a combination of gliding and rolling of the articular surfaces
against each other. However, unlike the knee, it is not possible to define the
extent of each type of motion within each of the various movements. Although
the range of movement at the shoulder joint is relatively large, the mobility
of the upper limb against the trunk is increased by movements of the pectoral
girdle. Indeed, the movements of flexion and extension, and abduction and
adduction, may be considered to be always accompanied by scapular and
clavicular movements, except perhaps for the initial stages. Shoulder joint
movement is more concerned with bringing the arm to the horizontal position,
while pectoral girdle movements, principally those of the scapula, are more concerned in bringing the arm into a vertical
position.
The association of shoulder and pectoral girdle
movement also increases the power of the movement. The rotator cuff muscles, being attached blose to the axes of movement,
have a poor mechanical advantage compared with muscles acting on the scapula, which are generally more
powerful as well as having considerable leverage. In patients with fused or
fixed shoulder joints a large degree of upper limb mobility with respect to the
trunk is still possible because of pectoral girdle movements.
In the following account shoulder joint
movements are considered initially with respect to the plane of the glenoid
fossa.
Flexion
and extension
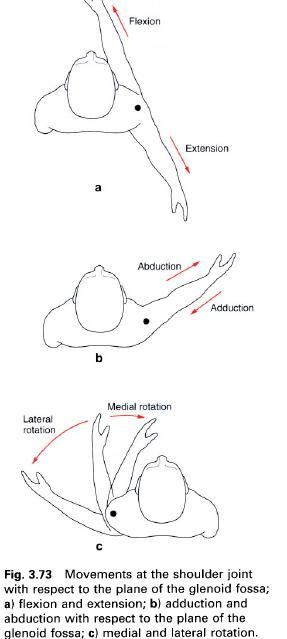
Flexion and extension occur about an axis
perpendicular to the plane of the glenoid fossa, so that in flexion the arm
moves forwards and medially at an angle of approximately 45° to the sagittal
plane(a). In extension it is carried backwards and laterally(a). The range of
flexion is approximately 110° and that of extension 70°. Both of these ranges
may be extended by movements of the pectoral girdle so that flexion of the
upper limb with respect to the trunk reaches 180° and extension just exceeds
90°. Extension is limited by the greater tubercle of the humerus coming into contact with the coracoacromial arch.
Flexion is produced by the anterior fibres of deltoid, clavicular head of pectoralis major, coracobrachialis and biceps.
Passive extension from the flexion position is essentially due to the eccentric
contraction of the above muscles. Beyond the neutral position, however,
extension is produced by the posterior fibres of deltoid, teres major and latissimus dorsi; to these may be added
the long head of triceps and the
sternal fibres of pectoralis major
when active extension is performed from a flexed position.
Abduction
and adduction
Abduction and adduction occur about an oblique
horizontal axis in the same plane as the glenoid fossa. In abduction the arm
moves anterolaterally away from the trunk(b). The total range of movement at
the shoulder joint is 120°; however only the first 25° occurs without
concomitant rotation of the scapula,
so that between 30° and 180° scapula rotation
augments shoulder abduction in the ratio of 1:2.
The terminal part of shoulder joint abduction
is accompanied by lateral rotation of the humerus.
This occurs not to prevent bony interlocking between the greater tubercle and
the acromion, but to provide further articular surface on the head of the humerus for the glenoid fossa. Abduction
of the medially rotated humerus is
limited by tension in the posterior capsule and the lateral rotators.
Adduction beyond the neutral position of the
joint is not possible because of the presence of the trunk. Abduction is
initiated by supraspinatus which,
although nowhere near as strong as deltoid,
is better placed to act on the humerus.
With the arm hanging at the side the fibres of deltoid, especially the middle fibres, run almost parallel to the humerus, so that on contraction they
pull the humerus upwards. Once the
arm has been pulled away from the side then deltoid
takes over and continues the movement. Supraspinatus
is required for the first 20° of abduction. If deltoid is paralysed, supraspinatus
is not functioning, deltoid cannot
initiate abduction. A passive abduction of some 20°, or learning to the
affected side so that the limb hangs away from the body, will enable deltoid to continue the movement. In
some circumstances biceps may be
re-educated to take over the initiating role of a paralysed supraspinatus. As abduction proceeds, teres major and minor hold the head of the humerus
down against the pull of the deltoid.
Together with subscapularis and infraspinatus, teres minor and major
stabilize the humeral head against the glenoid fossa.
Lateral rotation of the scapula accompanying abduction of the humerus is produced by the force-couple of the lower part of serratus anterior, acting on the
inferior angle of the scapula, and
the upper fibres of trapezius pulling
on the acromion process.
Adduction is produced by the eccentric contraction
of serratus anterior, trapezius, deltoid
and supraspinatus, under the action
of gravity. If adduction is resisted then a forceful movement is produced by pectoralis major, teres major, latissimus dorsi and coracobrachialis.
Medial
and lateral rotation
Rotation takes place about the longitudinal
axis through the humerus as described
earlier. In lateral rotation, it is the anterior surface of the humerus which is turned laterally(c). It
is produced It is produced by infraspinatus,
teres minor and the posterior fibrs of deltoid,
and has a maximum range of 80°. Medial rotation causes the anterior surface of
the humerus to be turned medially(c).
The maximum range of medial rotation in excess of 90°; however to reach this
value the forearm has to be pulled behind the trunk, otherwise contact between
the trunk and forearm limits the movements when the elbow is flexed. Medial
rotation is produced by subscapularis,
pectoralis major, latissimus dorsi, teres major and the anterior fibres of deltoid. The combined range of rotation
varies with the position of the arm, being greatest when the arm is by the
side, decreasing to 90° with the arm horizontal, and being negligible as the
arm approaches the vertical.
Rotation is limited by the extent of the
articular surfaces, and tension in the appropriate part of the joint capsule
and opposing musculature. Furthermore, it is the movement most commonly
affected by pathology or injury to the shoulder joint. When assessing the range
of rotation possible at the joint, the elbow must be flexed so as to exclude
the possibility of any pronatory or supinatory action of the forearm.
Movements
of the shoulder joint with respect to the cardinal planes of the body
Although movements of the shoulder joint have
been considered with respect to the plane of the glenoid fossa, it is often
more convenient to test the range of movement possible with respect to the
cardinal planes of the body.
Movements of the arm about a transverse axis
through the humeral head produce what are termed “flexion” and “extension”.
Strictly speaking these movements are a combination of flexion and abduction,
and extension and adduction – the degree of each component depending on the
orientation of the scapula on the
chest wall. The forward “flexion” movement has a range of 180° with scapula rotation. “Adduction” is the
combined movement of adduction and flexion.
Again the movement is limited by the trunk so
that adduction beyond the neutral position of the joint is not possible.
However, with protraction of the pectoral girdle some 30° of “adduction” is
possible as the arm is brought across the front of the chest. Similarly,
retraction of the pectoral girdle allows a minimal amount of “adduction” to
occur behind the back.
Although the terminology used to describe these
various movements of the arm at the shoulder joint is of little practical
significance, it is important to understand the context in which it is being
used. It is also important to be fully aware of which movements are being
tested when asking individuals to perform certain actions. Two simple
activities that demonstrate the mobility of the shoulder joint and pectoral
girdle are - combing the hair and
putting a coat on jacket.
With respect to the cardinal planes when the
arm is flexed at 45° and abducted 60° and neither medially nor laterally
rotated, it is said to be in the position of function of the shoulder. This
corresponds to the position of equilibrium of the short scapular muscles; hence
its use when immobilizing fractures of the humeral shaft.
Accessory
movements
When the subject is lying supping the muscles
around the shoulder are relatively relaxed. In this position the relative
laxity of the ligaments and joint capsule allow an appreciable range of
accessory movements. By placing the hand high up in the axilla and applying a
lateral force to the upper medial aspect of the arm, the head of the humerus can be lifted away from the
glenoid fossa by as much as 1cm.
Proximal and distal gliding movements of the
head of the humerus against the
glenoid fossa can be produced by forces applied along the shaft of the humerus. Similarly, anterior and
posterior gliding movements can be produced by applying pressure in an
appropriate direction, to the region of the surgical neck.
Palpation
The line of the shoulder joint cannot be
directly palpated due to the mass of muscles surrounding it. However, the
surface projection of the joint line can be estimated first by identifying the
surface projection of the midpoint of the joint. This latter point is
approximately 1cm lateral to the apex of the coracoid process. A vertical line,
slightly concave laterally, through this point gives an indication of the joint
line.
Biomechanics
The rotator
cuff muscles are active during abduction and lateral rotation, providing
stability at the shoulder joint. However, they are probably also involved in
the pathogenesis of dislocation of the shoulder. In any equilibrium analysis of
the joint certain assumptions have to be made. The following is based on an
account given by Morrey and Chao(1981). The assumptions these authors made
were:
- that each muscle contributing to the equilibrium acts with a force proportional to its cross-sectional area, this being 6.2kg/cm2;
- that each muscle is equally active;
- that the active muscle contracts along a straight line connecting the centres of its two areas of attachment.
While none of these assumptions is necessarily
true, they do provide a framework within which to work. When the unloaded arm
is laterally rotated and abducted to 90° there is a compressive force of
approximately 70kg between the articular surfaces, and anterior and inferior
shear forces of 12kg and 14kg respectively. These forces are produced by
muscles actively resisting the weight of the arm; the resultant force is
directed 12° anteriorly with a magnitude of 72kg.
If, as well as being abducted and laterally
rotated, the arm is also extended by 30° and loaded so that the muscles are
contracting maximally, then the magnitude of the various forces across the
joint increase dramatically. The compressive force across the joint is now of
the order of 210kg, while the anterior and inferior shear forces have increased
to 42kg and 58kg respectively. The resultant force is now directed 36°
anteriorly and has a magnitude of 222kg. To prevent anterior dislocation
occurring, the shearing forces must be balanced by the joint capsule and its
associated ligaments, because the glenoid fossa is too shallow to provide much
constraint. As the tensile strength of the capsule and ligaments is of the
order of 50kg, an imbalance of forces may occur leading to dislocation at the
joint. Once the anterior part of the capsule has been torn then less force is
required for subsequent dislocations to occur.
The above force analysis is comparable to the
situation when an individual slips when walking on ice and puts out his or her hand and arm to break a backward fall.
Velocity
of movement
With the shoulder joint being extremely mobile,
some of its movements are performed at fairly high velocities. In many
instances, for example when studying natural or artificial joints and their
lubrication, a knowledge of the sliding velocities at the articulating surfaces
is of importance.
Using cine film techniques and by suitable
trigonometric relationships the maximum sliding velocities at the shoulder
joint in various common activities have been determined. These are for hanging
clothes 100 mm/s, sweeping 34 mm/s, arm swing during walking 30 mm/s, eating 13
mm/s and dressing 25 mm/s. Obviously in activities requiring a fast and
forceful movement at the shoulder, such as the tennis serve, then the sliding
velocities will be much greater. The demands made upon the lubricating fluid
and articular surfaces in such situations are high. It is not surprising therefore
that sometimes the system breaks down and some form of joint trauma results.
Shoulder
joint replacement
Replacement of a damaged or arthritic humeral
head offers the immediate relief of pain. However, an intact rotator cuff and a normal glenoid fossa
are prerequisites for this type of replacement. The replacement, when used
following a severe fracture of the humeral head, should be done as soon as
possible, and certainly not later than four weeks following the injury, because
of the extensive development of scar tissue and the subsequent limitation of
motion.
Total shoulder implants have proved to be more
successful than replacement of the humeral head alone. If the rotator cuff is
deficient then a restrained shoulder implant will give stability as well as
relief of pain. It is not uncommon for the ball and socket of the joint to be
reversed, so that the socket is now on the humerus
and the ball on the scapula.







0 коментара:
Постави коментар