



Blood and nerve supply
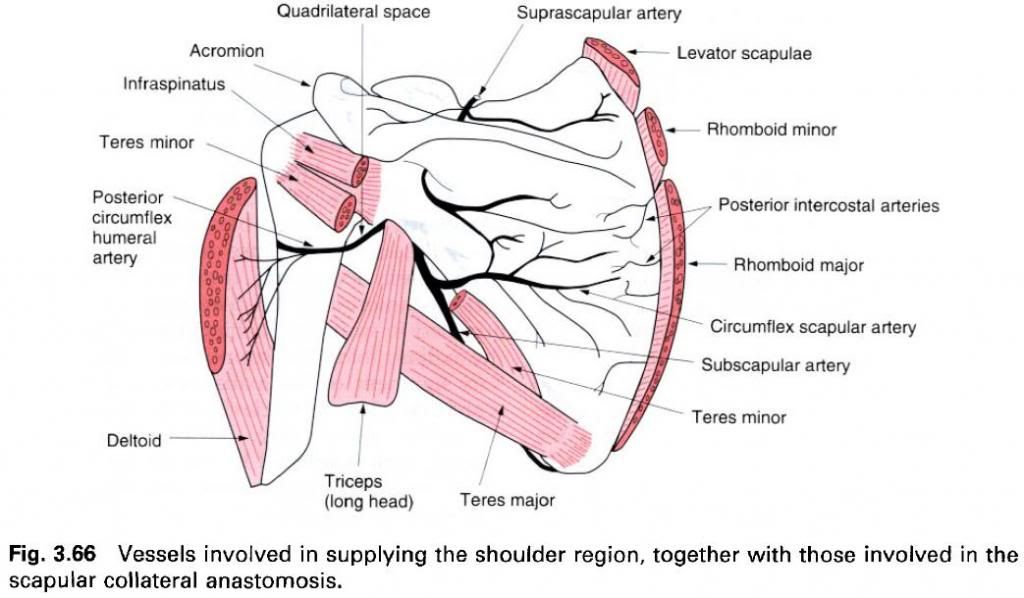
The arterial supply is from numerous sources as
there is an important anastomosis around the scapula involving vessels from the subclavian and axillary arteries
and the descending aorta. The supply to the shoulder joint is by branches from
the suprascapular branch of the subclavian artery, the acromial branch of the
thoracoacromial artery, and branches from the anterior and posterior circumflex
humeral arteries. The latter three are all branches of the axillary artery. The
venous drainage is by similarly named veins which drain into the external
jugular and axillary veins.
Lymphatic drainage of the joint is to the lymph
nodes within the axilla, eventually passing by the apical group of nodes into
the subclavian lymph trunk.
The nerve supply to the shoulder joint is by
twigs from several nerves which pass close to the joint. The twigs come from
the suprascapular, axillary, subscapular, lateral pectoral and musculocutaneous
nerves, and have a root value of C5, 6 and 7.
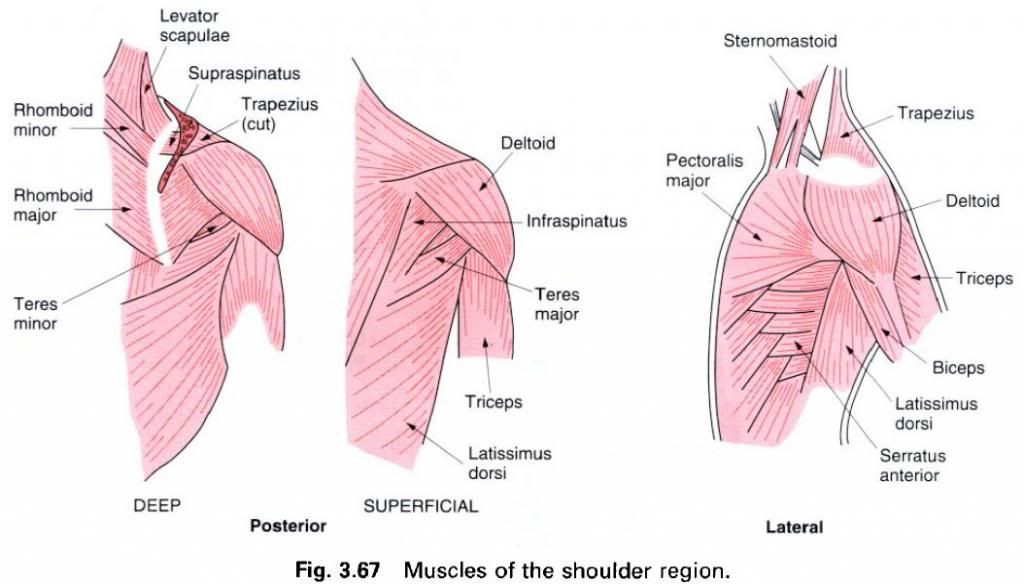
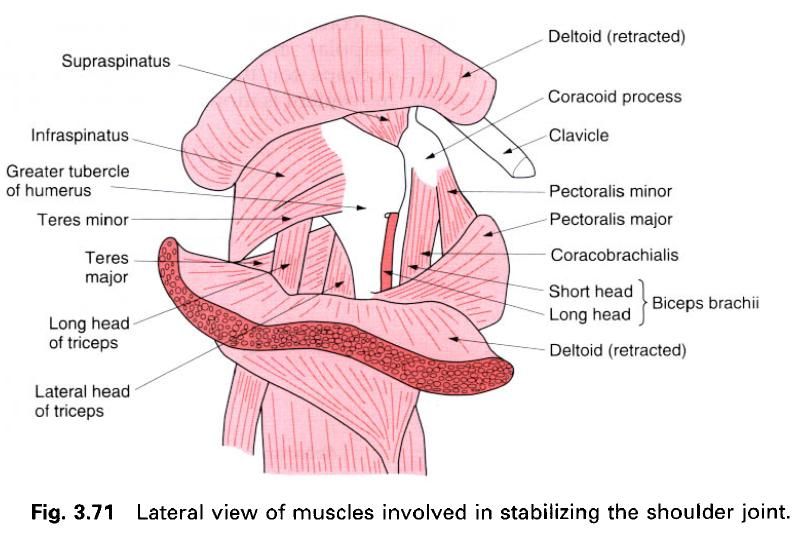
Relations
The shoulder joint is almost completely
surrounded by muscles passing between the pectoral girdle and the humerus. They serve to protect the joint
by helping to suspend the upper limb from the pectoral girdle and so convey
some degree of stability to the joint. Some muscles are more important in this
respect than others. The anterior, superior and posterior parts of the joint
are directly related to the tendons of subscapularis,
supraspinatus, and infraspinatus and teres minor respectively. These tendons all blend with the humeral
part of the joint capsule, and because of their action on the shoulder joint,
have become known as rotator cuff.
Covering the superolateral part of the joint is deltoid, giving the shoulder its rounded appearance. The greater
and lesser tubercles of the humerus
can be palpated through deltoid, as
can the long head of biceps as it
emerges from within the capsule. The tendon of the long head of biceps passes directly above the joint
within the capsule. Superiorly, and separated from the joint by the tendon of supraspinatus, is the coracoacromial
arch. Inferiorly, coming from the infraglenoid tubercle, is the long head of triceps as it passes into the arm almost
parallel to the humerus.
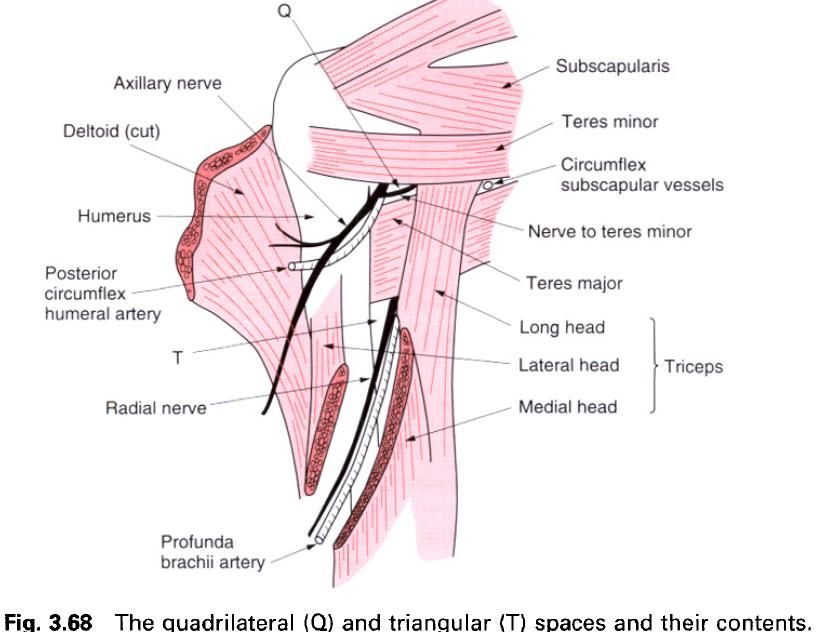
Immediately below the shoulder joint is the
quadrilateral space, bounded superiorly by teres minor, inferiorly by teres major,
medially by the long head of triceps
and laterally by the shaft of humerus.
Passing through this space from anterior to posterior are the axillary nerve
and posterior circumflex humeral artery. Downward dislocation of the head of
the humerus or prolonged upwardly
applied pressure, for example as when falling asleep with the arm hanging over
the back of a chair, may cause temporary or permanent damage to the nerve and
consequent loss of function of deltoid
and teres minor. Immediately medial
to the quadrilateral space is a triangular space, bounded by teres minor and major and the long head of triceps
through which pass the circumflex scapular vessels. A further triangular space
is found below the quadrilateral space. This has the long head of the triceps as its medial border, the shaft
of the humerus laterally and the
lower border of teres major as its
base. It is an important space as the radial nerve and the profunda brachii
vessels pass through it to the posterior compartment of the arm. Fractures of
the shaft of the humerus, or pressure
from the axillary pad of an incorrectly used crutch, may involve the radial
nerve, resulting in radial nerve palsy, that is wrist drop, which will affect
the functional use of the hand.
The axilla
Inferomedial to the shoulder joint is the
pyramidal-shaped axilla – the space between the arm and the thorax which
enables vessels and nerves to pass between the neck and the upper limb(a). The
apex of the axilla is formed by the clavicle
anteriorly, scapula posteriorly and
outer border of the first rib medially. Its concave base or floor is formed by
deep fascia extending from the fascia over serratus anterior to the deep fascia of the arm, attached in front and behind to the
margins of the axillary folds and supported by the suspensory ligament of the
axilla, which is a downward extension of the clavipectoral fascia below pectoralis minor(b). The anterior
axillary wall is formed by pectoralis major, its lower rounded fold formed by the twisting nature of the muscle
fibres as they pass from the chest wall to the humerus. The posterior wall, which extends lower than the anterior,
is formed by subscapularis and teres major, with the tendon of latissimus dorsi twisting around teres major(b). The medial wall is
formed by serratus anterior, and the
lateral wall by the floor of the intertubercular groove(c). Both the anterior
and posterior axillary folds can be readily palpated. A vertical line midway
between them, running down the thoracic wall, is the midaxillary line.
When the arm is fully abducted the axillary
folds virtually disappear as the muscles forming them run almost parallel to
the humerus. Indeed, the axillary
hollow may be replaced by a bulge.
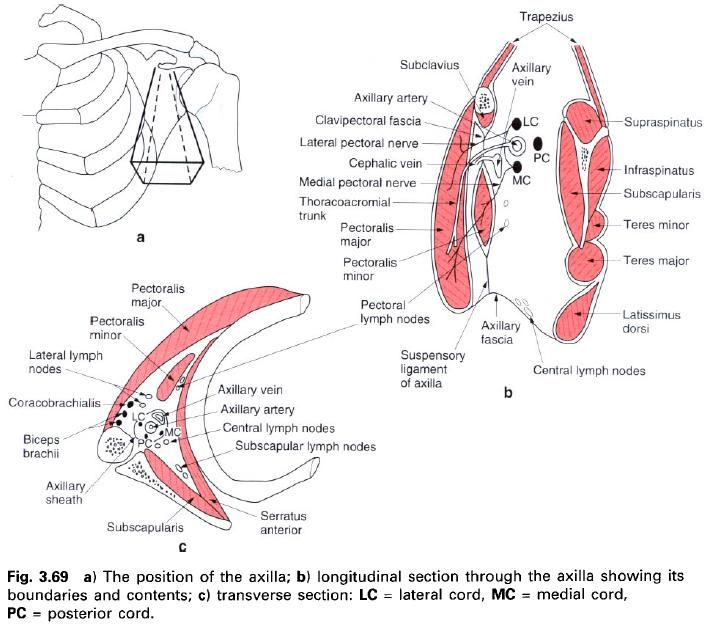
The principal contents of the axilla are the
blood vessels and nerves which pass between the neck and the upper limb(b,c).
These are the axillary artery and its branches, the corresponding vein and its
tributaries, and the branches of the brachial plexus. Together, with the
various groups of lymph nodes, they are surrounded by fat and loose areolar tissue. The tendon of long head of biceps runs in the intertubercular
groove, and so is just within the axilla. Also within the axilla are the short
head of biceps and coracobrachialis. The major vessels and
nerve trunks are enclosed within the axillary sheath, a fascial extension of
the prevertebral layer of cervical fascia. The axillary sheath is adherent to
the clavipectoral fascia behind pectoralis minor, and just beyond the second
part of the axillary artery blends with the tunica adventitia of the vessels.
The axillary artery runs through the axilla,
being posterior and superior to the vein, and can be indicated on the surface
of the abducted arm by a straight line running from the middle of the clavicle to the medial prominence of coracobrachialis. With the arm hanging
by the side, the artery describes a gentle curve with the concavity facing
inferomedially.
The artery is crossed anteriorly by the tendon
of pectoralis minor, which serves to
divide it into three parts. Above the first part of the artery lie the lateral
and posterior cords of the brachial plexus, and behind it is the medial cord –
it is crossed by a communicating loop between the medial and lateral pectoral
nerves. The second part of the axillary artery, behind pectoralis minor, has the various cords of the brachial plexus in
their named positions. The third part of the artery, lying laterally against coracobrachialis, has the
musculocutaneous nerve laterally, the median nerve anteriorly, the ulnar and
medial cutaneous nerves of the arm and forearm medially, and the axillary and
radial nerves posteriorly.
The axillary lymph nodes are widely distributed
within the axillary fat, but may be
conveniently divided into five groups(b,c). The lateral nodes lie along and
above the axillary vein and receive the majority of the lymphatic drainage of
the upper limb. The subscapular(posterior) nodes lie along the subscapular
artery and receive lymph from the scapular region and back above the level of
the umbilicus. The pectoral nodes, along-side the lateral thoracic artery,
receive lymph from the anterior chest wall including the breast. These groups
of nodes draing to a central group, which lie above the axillary floor. From
here efferents pass to the apical group of nodes(the only group lying above the
tendon of pectoralis minor) and thence to the subclavian lymph trunk.
Because of the involvement of the axillary
nodes in the lymphatic drainage of the breast, they may be subjected to
radiotherapy treatment in an attempt to limit the secondary spread of cancer
from the breast. It is important to remember that the lateral group of nodes
lie above the axillary vein so that they can be excluded from the treatment programmes,
otherwise severe problems with the lymphatic drainage of the upper limb may
result.
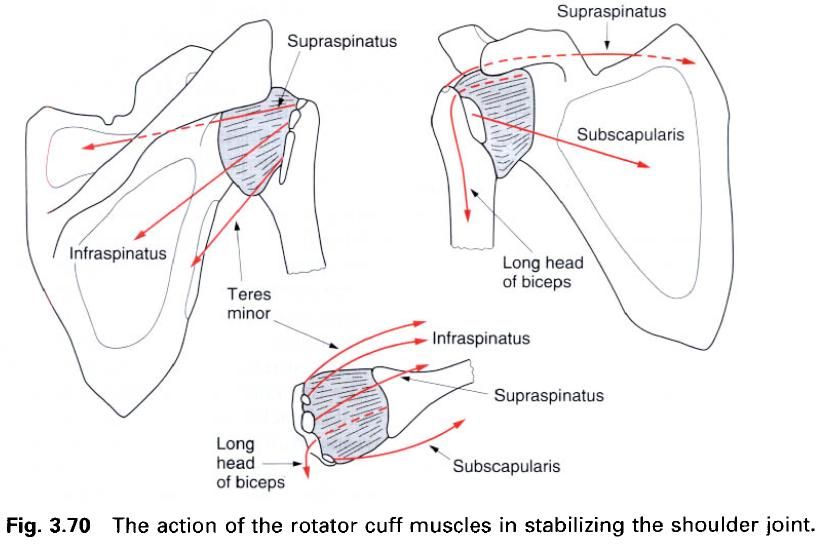
Stability
The incongruity of the articular surfaces,
together with the laxness of the joint capsule, suggest that the shoulder joint
is not very stable. Although dislocation of the shoulder is rather common it is
by no means an everyday occurrence. What factors are responsible for conferring
stability on the joint? The glenoid labrum, as well as deepening the fossa,
also makes the joint surfaces more congruent, and thus becomes a significant
stabilizing factor. Fracture of the glenoid or tearing of the labrum often
results in dislocation.
Perhaps the most important factor, however, is
the tone in the short scapular(rotator cuff) muscles. Not only do these muscles(supraspinatus, infraspinatus, teres minor
and subscapularis) attach very close
to the joint, but they fuse with the lateral part of the capsule. In this way
they act as ligaments of variable length and tension, and also prevent the lax
capsule and its synovial lining from being trapped between the articulating
bones. The inferior part of the capsule is the weakest, being relatively
unsupported by muscles. However, as the arm is gradually abducted, the long
head of triceps and teres major become increasingly applied
to this aspect of the joint.
In addition to the rotator cuff muscles, all
the muscles passing between the pectoral girdle and the humerus assist in maintaining the stability of the joint. Particularly
important are the long heads of triceps
and biceps. The tendon of the long
head of biceps, being partly
intracapsular, acts as a strong support over the superior part of the joint.
The long head of triceps gives
support below the joint when the arm is abducted.
An upward displacement of the head of the humerus is resisted by the overhanging
coracoacromial arch. Although not part of the joint, this arch, separated from
the joint by the subacromial bursa, functions mechanically as an articular
surface. The arch is so strong that an upward thrust on the humerus will fracture either the clavicle or the humerus first before compromising the arch.
Dislocation of the shoulder is more common than
for many joints, being favoured by the need to have the joint as mobile as
possible. In addition, the long humerus
has great leverage in dislocating forces. In anterior dislocation, which is
more common, the head of the humerus comes to lie under the coracoid process producing a bulge in the region of the
clavipectoral groove. At the same time the roundness of the shoulder is lost.
In such dislocations, the humeral head usually comes through the joint capsule
between the long head of triceps and
the inferior glenohumeral ligament.
Because the glenoid fossa faces
anterolaterally, it is better situated to resist posteriorly directed forces.
The presence of infraspinatus and teres minor also reinforces the capsule
posteriorly. Posterior dislocation may result when a large force is applied to
the long axis of the humerus when the
arm is medially rotated and abducted. The joint capsule tears in the region of teres minor with the head of the humerus coming to lie below the spinous
process of the scapula.












0 коментара:
Постави коментар