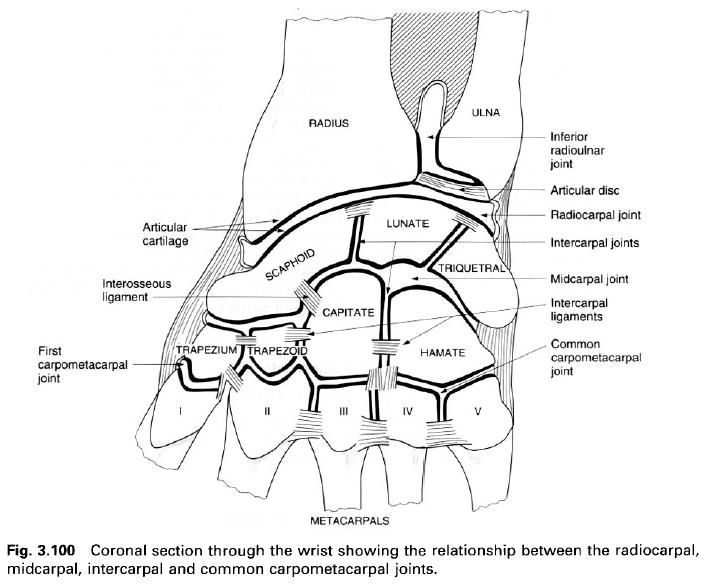
The radiocarpal joint is formed between the
distal surfaces of the radius and the
articular disc, and the scaphoid, lunate and triquetral of the proximal row of
carpal bones. It is a synovial joint of the ellipsoid type allowing movement in
two planes.
Articular surfaces
Distal
surface of the radius and articular
disc
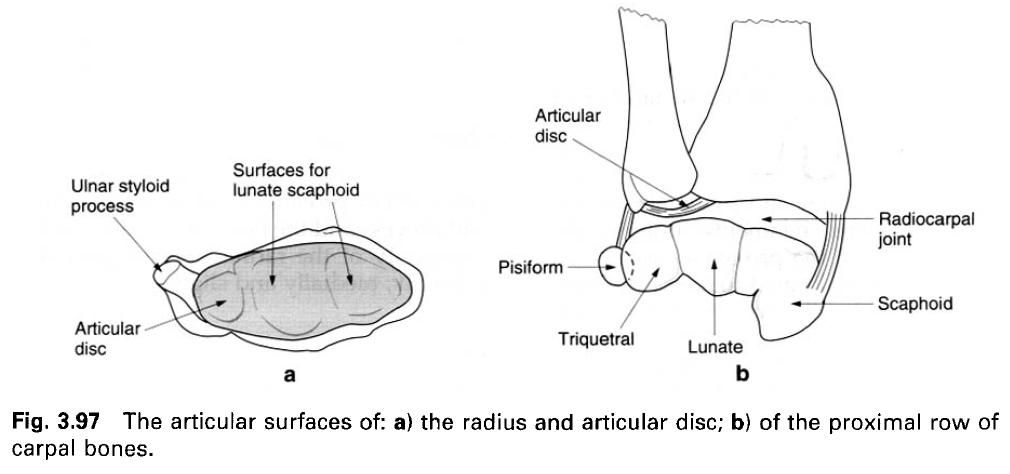
The radius
and articular disc form a continuous, concave ellipsoid surface, being
shallower in its transverse long axis than in its shorter anteroposterior
axis(a). The articular cartilage on the radius
is divided by a low ridge into a lateral triangular and a medial quadrangular
area.
Proximal
carpal row
The proximal row of carpal bones presents an
almost continuous convex articular surface(b). The three carpal bones are
closely united by interosseus ligaments which are continuous with the cartilage
on the proximal surfaces of the bones. In the anatomical position, the scaphoid
lies opposite the medial radial area and the articular disc, and the triquetral
is in contact with the medial part of the joint capsule(b).
Joint
capsule and synovial membrane
A fibrous capsule completely encloses the
joint. It is attached to the distal edges of the radius and ulna
anteriorly and posteriorly. Laterally and medially it is attached to the radial
and ulnar styloid processes respectively. Distally the capsule is firmly
attached anteriorly and posteriorly to the margins of the articular surfaces of
the proximal row of carpal bones. Medially it passes to the medial side of the
triquetral, and laterally to the lateral side of the scaphoid. Both the
anterior and posterior parts of the capsule are thickened and hence
strengthened, while at the sides it blends with the collateral ligaments.
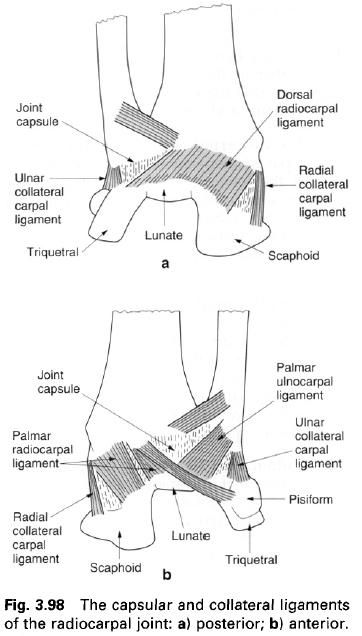
Capsular
ligaments
The capsular ligaments are distinct bands of
fibres passing between specific bones. As well as strengthening the capsule,
their arrangement determines that the hand follows the radius in its movements and displacements.
Dorsal
radiocarpal ligament. The
dorsal radiocarpal ligament extends from the posterior edge of the lower end of
the radius to the posterior surface
of the scaphoid, lunate and triquetral(a). Its fibres run downwards and
medially, principally to the triquetral, and are continuous with the dorsal
intercarpal ligaments.
Palmar
radiocarpal ligament. The
palmar radiocarpal ligament is a broad band of fibres passing downwards and
slightly medially from the anterior edge of the lower end of the radius and its styloid process, to the
anterior surfaces of the proximal row of carpal bones(b). Some of the fibres
are prolonged and extend to attach to the capitate.
Palmar
ulnocarpal ligament. The
palmar ulnocarpal ligament is formed by fibres extending downwards and
laterally from the anterior edge of the articular disc and the base of the
ulnar styloid process to the anterior surfaces of the proximal carpal bones(b).
These anterior and posterior capsular ligaments
become taut in extension and flexion of the radiocarpal joint respectively.
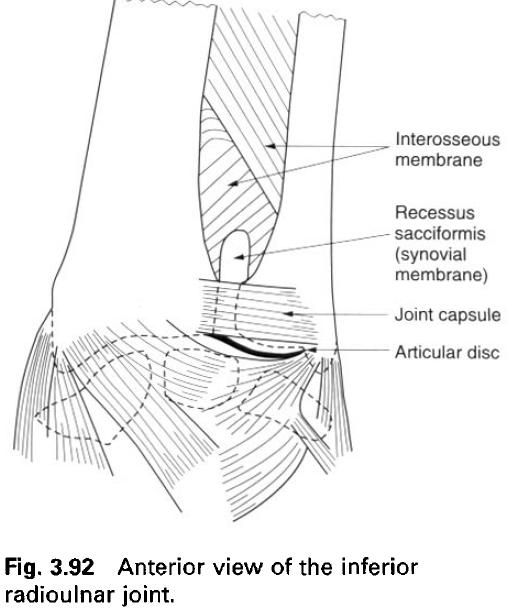
Synovial
membrane
A relatively lax synovial membrane lines the
deep surface of the joint capsule attaching to the margins of all the articular
surfaces. It presents numerous folds, particularly posteriorly. Because of the
presence of the articular disc of the inferior radioulnar joint and the
completeness of the interosseus
ligaments uniting the proximal surfaces of the proximal carpal row, the
synovial cavity is limited to the radiocarpal space. Only occasionally does it
communicate with the inferior radioulnar joint by a perforation in the
articular disc, or with the intercarpal joint when one of the interosseus
ligaments is incomplete.
Ligaments
At the sides of the radiocarpal joint,
collateral ligaments reinforce and strengthen the joint capsule. They are
active in limiting abduction and adduction at the joint. In adduction, the
radial ligament becomes taut while the ulnar relaxes; in abduction the reverse
occurs.
Radial
collateral carpal ligament
The radial collateral carpal ligament passes
from the tip of the radial styloid process to the lateral side of the scaphoid,
immediately adjacent to its proximal articular surface, and to the lateral side
of the trapezium.
Ulnar
collateral carpal ligament
The ulnar collateral carpal ligament is a
rounded cord attached to the ulnar styloid process above and to the base of the
pisiform and the medial and posterior non-articular surfaces of the triquetral
below. By its attachment to the pisiform the ligament also blends with the
medial part of the flexor retinaculum.
Blood and nerve supply
The arterial supply to the joint is by branches
from the dorsal and palmar carpal networks, with venous drainage going to the
deep veins of the forearm. Lymphatic drainage of the joint follows the deep
vessels.
The nerve supply to the joint is by twigs from
the anterior interosseus branch of the radial nerve, the posterior interosseus
branch of the radial nerve, and the dorsal and deep branches of the ulnar
nerve, with root value C7, 8.
Surface making
The position of the joint is indicated by a
line, slightly convex proximally, between the radial styloid process and the
head of the ulna, so that the
concavity of the radius and articular
disc face distally, medially and slightly anteriorly.
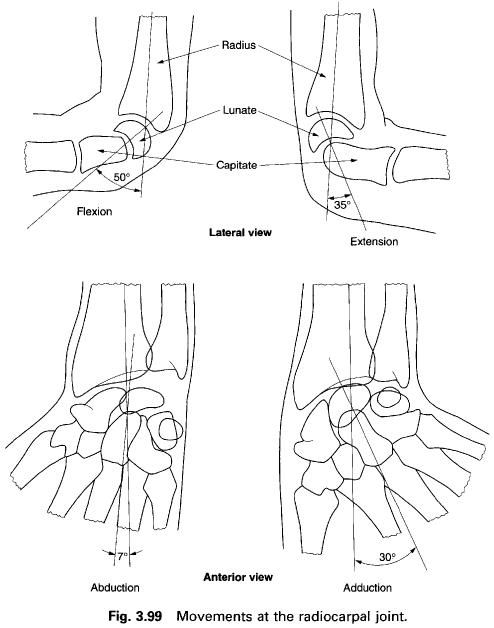
Movements
Movements of flexion and extension; and
adduction and abduction are possible at the radiocarpal joint. However, each of
these is also contributed to by movements between the proximal and distal row
of carpal bones at the midcarpal joint.
Flexion
and extension
Flexion and extension occur about a transverse
axis more or less in the sagittal plane such that the hand moves towards the front of the forearm in flexion and
towards the back of the forearm in extension. Flexion is freer than extension
and has a maximum range of 50°, whereas extension has a maximum range of 35°.
The movements are checked by the margins of the radius, and because the posterior margin extends further distally
than the anterior, extension is checked earlier than flexion.
In flexion the scaphoid and lunate move within
the concave distal end of the radius
so that their proximal surfaces face postero-superiorly. In addition the
scaphoid twists about its long axis so that its tubercle becomes less prominent
in full flexion. During extension the twisting of the scaphoid about its long
axis makes the tubercle more prominent in full extension.
Abduction
and adduction
Abduction and adduction, also reffered to as
radial and ulnar deviation, are lateral or medial movements respectively of the
proximal row of carpal bones in relation to the distal end of the radius. The radial styloid process
extends further distally than the ulnar styloid process. Consequently,
abduction is more limited at the radiocarpal joint having a range of only 7°,
whereas adduction has a range of 30°. In adduction the scaphoid rotates so that
its tubercle moves away from the radial styloid process, enabling the lunate to
move laterally so that it comes to lie entirely distal to the radius. The triquetral lies distal to
the articular disc. In abduction the triquetral moves medially and distally to
be clear of the radius; the lunate
follows so that its centre lies distal to the inferior radioulnar joint. The
movement is limited by impact of the scaphoid tubercle on the radial styloid
process.
Accessory
movements
An anteroposterior gliding of the proximal row
of carpal bones against the radius
and articular disc can be produced by firmly gripping the lower end of the radius and ulna with one hand, and
the proximal row of carpal bones with the other. Alternate anterior and posterior
pressure elicits a palpable gliding movement at the radiocarpal joint. With the
same grip, a longitudinally applied force along the line of the forearm pulls
the carpal bones away from the radius
and articular disc.