



The synovial acromioclavicular joint connects
the clavicle with the shoulder blade.
The role that this joint plays in the movement of the pectoral girdle is
considered by some to be greater than that of the sternoclavicular joint,
particularly for movements in or close to the sagittal plane.
Articular
surfaces
The articulation is between an oval flat or
slightly convex facet on the lateral end of the clavicle, and a similarly shaped flat or slightly concave facet on
the anteromedial border of the acromion process. Both joint surfaces are
covered with fibrocartilage. The major axis of both facets runs from
anterolateral to posteromedial, so that the clavicular facet faces laterally
and posteriorly, and that on the acromion faces medially and anteriorly.
Consequently, the lateral end of the clavicle
tends to over-ride the acromion, which together with the slope of their
articulating surfaces favours displacement of the acromion downwards and under
the clavicle in dislocations.
Joint
capsule and synovial membrane
A relatively loose fibrous capsule surrounds
the joint attaching to the articular margins. Its strong coarse fibres run in
parallel fasciculi from one bone to the other. The capsule is thickest and
strongest above where it is reinforced by the fibres of trapezius. Some authorities contend that the joint capsule is
reinforced by two strong ligaments, the superior and inferior acromioclavicular
ligaments, passing between the adjacent surfaces of the two bones. In reality
these are no more than capsular thickenings, which will show varying degrees of
thickening in different individuals.
Synovial membrane lines the inner surface of
the capsule attaching to the margins of the articular surfaces.
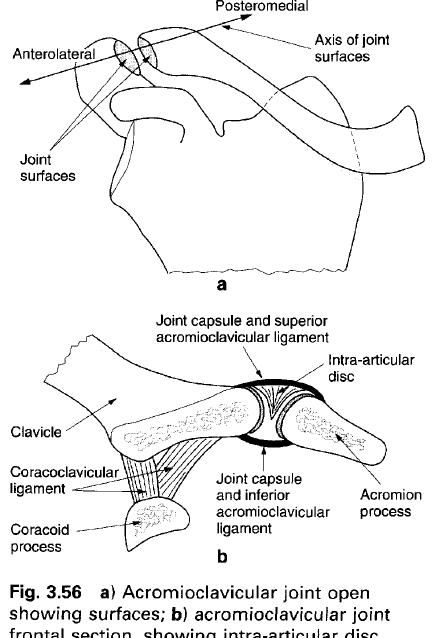
Intra-articular
surfaces
A wedge-shaped, fibrocartilaginous articular
disc partially divides the cavity in most joints. When present, the disc is
attached to the upper inner part of the capsule and dips down between the two
articulating surfaces. Only rarely does the disc form a complete partition
within the joint. The presence of the articular disc partially compensates for
the small degree of incongruity between the two joint surfaces.
Ligaments
Apart from the capsular thickening alluded to
above, the strength of the acromioclavicular joint is provided by an
extracapsular accessory ligament, the coracoclavicular ligament.
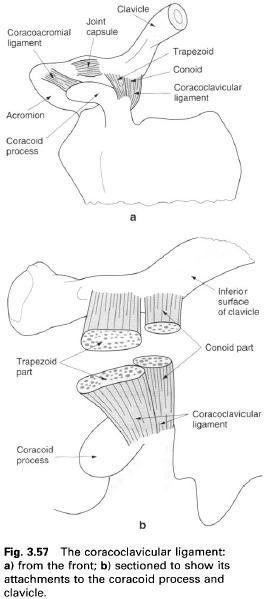
Coracoclavicular
ligament
The coracoclavicular ligament is extremely
powerful, anchoring the lateral end of the clavicle
to the coracoid process. The ligament, which is medial to the acromioclavicular
joint, stabilizes the clavicle with
respect to the acromion. It is in two parts which are named according to their
shapes, these being the posteromedial conoid
and anterolateral trapezoid
ligaments. The two parts tend to be continuous with each other posteriorly but
are separated anteriorly by a small gap in which is found a synovial bursa.
The apex of the fan-shaped conoid ligament is
attached posteromedially to the “elbow” of the angulated coracoid process. From
here the ligament broadens as it passes upwards, more or less in the frontal
plane, to attach to the conoid tubercle on the under surface of the clavicle.
The stronger and more powerful trapezoid
ligament is a flat quadrilateral band. It is attached inferiorly to a roughened
ridge on the upper surface of the coracoid process. The wider superior surface
of the ligament is attached to the trapezoid line on the under surface of the clavicle, which runs anterolaterally
from the conoid tubercle. Although the two surfaces of the trapezoid ligament
are set obliquely, the ligament lies more or less in the sagittal plane, being
more nearly horizontal than vertical.
Because the conoid and trapezoid ligaments lie
in different planes, which are more or less at right angles to each other, and
because the posterior edge of the trapezoid ligament is usually in contact with
the lateral edge of the conoid ligament, a solid angle facing anteromedially is
formed between them.
The two parts of the coracoclavicular ligaments
are set so as to restrain opposite movements of the scapula with respect to the clavicle.
The conoid ligament limits forward movement of the scapula, while the trapezoid limits backward movements. The
importance of these limiting movements will be discussed more fully in the
section on movements of the pectoral girdle. Both ligaments, but especially the
trapezoid ligament, prevent the acromion being carried medially under the
lateral end of the clavicle when
laterally directed forces are applied to the shoulder.
Blood and nerve supply
The arterial supply to the joint is by branches
from the suprascapular branch of the subclavian and acromial branch of the
thoracoacromial trunk. Venous drainage is to the external jugular and axillary
veins. Lymphatic drainage will be to the apical group of axillary nodes.
The nerve supply to the joint is by twigs from
the lateral supraclavicular, lateral pectoral, suprascapular and axillary
nerves, from roots C4, 5 and 6.
Relations
The attachments of trapezius and deltoid
cover the posterosuperior and anterosuperior aspects of the joint respectively.
Medial to the coracoclavicular ligament the transverse superior scapular
ligament converts the scapula notch
into a foramen. The suprascapular vessels pass above the ligament, while
beneath it and through the foramen runs the suprascapular nerve. The lateral
supraclavicular nerve crosses the clavicle
medial to the acromioclavicular joint.
Although not directly associated with the
joint, the coracoacromial ligament, as its name suggests, is attached to both
the coracoid and acromion process.
Stability
The stability of the joint is essentially
provided by the coracoclavicular ligament. Trapezius
and deltoid by virtue of their
crossing the joint will also provide a certain amount of stability during
movement of the joint.
Movement
The movements of the joint are entirely passive
as there are no muscles connecting the bones which could cause one to move with
respect to the other. Muscles which move the shoulder blade cause it to move on
the clavicle. Indeed, all movements
of the shoulder blade involve movement at both the acromioclavicular and
sternoclavicular joints. All movements at the acromioclavicular joint, except
that of axial rotation, are gliding movements with the coracoclavicular
ligament acting so as to limit these movements.
The acromioclavicular joint has three degrees
of freedom of motion about three axes. These movements are probably best
described in terms of their relation to the shoulder blade rather than with respect
to the cardinal axes of the body, since the joint constantly changes its
relation to the trunk. The most important function of the joint is that it
provides an additional range of movement for the pectoral girdle after the
range of movement at the sternoclavicular joint has been exhausted.
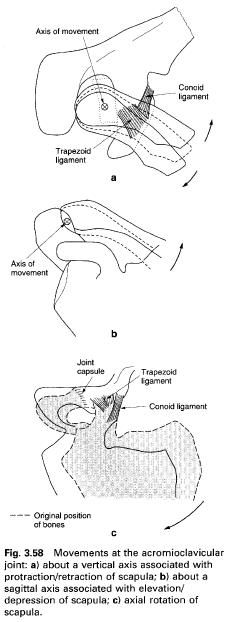
Movement
about a vertical axis(a)
This movement is associated with protraction
and retraction of the shoulder blade. The axis of movement passes vertically
through the lateral end of the clavicle
midway between the joint and the coracoclavicular ligament. As the acromion
glides backwards with respect to the clavicle,
the angle between the clavicle and
shoulder blade increases: similarly as the acromion glides forwards this angle
decreases. Backward movement of the acromion is checked by the anterior joint
capsule and actively limited by the trapezoid ligament as it becomes stretched.
Forward movement will be checked by the posterior joint capsule and limited by
the stretching of the conoid ligament. Towards the end of forward movement of
the acromion, the trapezoid ligament may also be put under tension and
therefore help to limit the movement. Compensatory movements of the clavicle at the sternoclavicular joint
accompany these actions at the acromioclavicular joint.
Movement
about a sagital axis(b)
Movement about this axis occurs when the
shoulder blade is elevated or depressed. It has been estimated that the total
range of movement about this axis is no more than 15°. Elevation is limited by
tension developed in both parts of the coracoclavicular ligament, with the
conoid ligament becoming stretched first; depression is checked by the coracoid
process coming into contact with the under surface of the clavicle.
Axial
rotation(c)
Axial rotation at the acromioclavicular joint
is associated with medial and lateral rotation of the shoulder blade, that is
when the glenoid fossa faces inferiorly or superiorly respectively. The range
of rotation of the shoulder blade with respect to the clavicle is of the order of 30°, and occurs about an axis that
passes through the conoid ligament and the acromioclavicular joint. The
movement allows the flexed arm to be fully elevated. Restraints to rotation are
provided by both parts of the coracoclavicular ligament.
Accessory
movements
With the subject lying supine, downward
pressure applied with the thumb on the lateral end of the clavicle causes it to glide backward against the acromion process.
Palpation
The line of the acromioclavicular joint can be
palpated from above by applying a downward pressure to the lateral end of the clavicle.






0 коментара:
Постави коментар