



The superficial fascia
The superficial fascia of the upper limb shows
regional differences between, for example, the shoulder region and the hand. In the shoulder region and arm, it
contains a variable amount of fat. In
the female there is a deposition of fat
in this region – a secondary sexual characteristic, the amount of which tends
to increase after middle age. At the elbow, a subcutaneous bursa is present
between the skin and the olecranon process. This may become enlarged in people
who often tend to lean on their elbows, giving rise to a condition known as
“student’s elbow”.
There is nothing particularly noteworthy about
the superficial fascia in the forearm. However, in the hand there are several specializations, most of which enhance the
hand’s tactile or prehensile capabilities. On the dorsum of the hand the fascia is loose and thin, and
can be readily lifted away from the underlying tissue. It is in the palm of the
hand, as well as the palmar surface
of the digits where specializations of the fascia can be seen. In the centre of
the palm, strong bands of connective tissue connect the skin to the palmar
aponeurosis, which is a thickening of the deep fascia. Overlying the thenar and
hypothenar regions the fixation of the skin to the deep fascia is less well
marked, but here the superficial fascia is thicker and less fibrous to
facilitate the gripping action of the hand.
This is because it can adapt to the contours of the object being held. Palmaris
brevis lies in the superficial fascia over the hypothenar eminence. By
wrinkling the skin, it improves the grip. Similar less fibrous pads of tissue
are also found opposite the metacarpophalangeal joints, where the superficial
transverse metacarpal ligament(a band of transverse fibres) connects to the
palmar surfaces of the fibrous flexor sheaths of the fingers.
The pads on the palmar surfaces of the distal
phalanges are highly specialized regions which house numerous tactile nerve
endings. Here the skin is firmly attached to the latter two-thirds of the
distal phalanx. However, the blood
supply to the distal phalanx itself runs through this highly specialized pad.
If the pad becomes infected there may be compression of the artery with death
of this part of the bone. On the dorsum of the distal phalanx is the nail and
there is no superficial fascia deep to it.
The deep fascia
The deep fascia of the upper limb is continuous
with that of the upper back, and consequently can be traced superiorly to the
superior nuchal line on the occipital bone, to the ligamentum nuchae centrally
in the cervical region, and to the supraspinous and interspinous ligaments in
the thoracic region. In the shoulder region, the deep fascia is extremely
strong over infraspinatus and teres minor, being firmly attached to
the medial and lateral borders of the scapula.
Superiorly, a sheath is formed for deltoid,
which attaches to the clavicle, and
the acromion process and spine of the scapula.
The deep fascia covering pectoralis major attaches above to the clavicle, and may be traced, via the clavicle, to the neck. Inferiorly, it is continuous with the fascia
of the anterior abdominal wall. Medially, the fascia is firmly attached to the
sternum, whereas laterally it becomes thickened as the axillary fascia, which
forms the floor of the axilla. Further laterally it becomes continuous with the
deep fascia of the arm.
Deep to pectoralis major is the clavipectoral fascia. Medially, this is attached to the first
costal cartilage and passes to the coracoid process and coracoclavicular
ligament laterally. The clavipectoral fascia splits to surround subclavius
superiorly, and thus attaches to the undersurface of the clavicle. It also splits to enclose pectoralis minor inferiorly. An extension of the fascia from the
lateral border of pectoralis major
passes into the axilla and attaches to the axillary floor. This is often
referred to as the suspensory ligament of the axilla. The deep surface of the
clavipectoral fascia is connected to the axillary sheath surrounding the axillary
vessels and brachial plexus.
In the arm, the deep fascia forms an investing
layer around the muscles. It attaches at the elbow to the medial and lateral
epicondyles of the humerus and the olecranon process, becoming continuous with
the deep fascia of the forearm. Two intermuscular septa arise from the deep
surface of this investing layer and pass to attach to the supracondylar ridges
of the humerus. Both the medial and
lateral intermuscular septa are found only in the lower half of the arm.
Besides separating the arm into flexor and extensor compartments they also give
attachment to muscles in each compartment. Of the two, the medial intermuscular
septum is said to be the stronger.
In the forearm, the deep fascia of the elbow is
very strong because many of the muscles arising from either the common flexor
or extensor tendons also arise from the overlying fascia. The bicipital
aponeurosis helps to strengthen the fascia anteriorly, while the triceps insertion does so posteriorly.
The deep fascia is also strong and thick where it attaches to the posterior
border of the ulna, because it gives attachment to flexor digitorum profundus, and flexor
and extensor carpi ulnaris.
However, the fascia becomes thinner as it approaches the wrist, although at the
wrist there are two thickenings of the transverse fibres forming the flexor and
extensor retinaculae. These serve to hold the tendons entering the hand in
place and prevent “bowstringing”.
The flexor retinaculum
The flexor retinaculum is found anterior to the
carpus where it acts as a strong band
for retention of the long flexor tendons, converting the carpal sulcus into a
tunnel. It attaches laterally to the tubercle of the scaphoid and to both lips
of the groove on the trapezium, and medially to the pisiform and the hook of
the hamate. Flexor carpi radialis
passes below the flexor retinaculum in its own lateral compartment surrounded
by its synovial sheath. Medial to it, the single tendon of flexor pollicis longus is present, lying within its synovial
sheath. All eight tendons of flexor digitorum superficialis and profundus
run below the retinaculum in a common synovial sheath. The median nerve also
enters the hand by passing below the flexor retinaculum, where it lies in front
of the superficial tendons. It is here that it may become compressed if the
synovial sheaths become inflamed, thus giving rise to the “carpal tunnel
syndrome”.
In the palm of the hand there are two layers of fascia. The deeper layer covers the interossei and encloses adductor pollicis. The more superficial
layer is strong in its central part forming the palmar aponeurosis. On each
side of this, the fascia thins out to cover the thenar and hypothenar muscles.
The palmar aponeurosis strengthens the hand
for gripping, yet also protects the underlying vessels and nerves. It is a
dense, thick triangular structure bound to the overlying superficial fascia.
The apex is at the wrist and its base at the webs of the fingers. From the base
four slips pass into the fingers to become continuous with the digital sheaths
of the flexor tendons. Each slip further divides and has attachments to the
deep transverse metacarpal ligament, the capsule of the metacarpophalangeal
joint and the sides of the proximal phalanx. The slips cross in front of the lumbricals, and the digital vessels and
nerves.
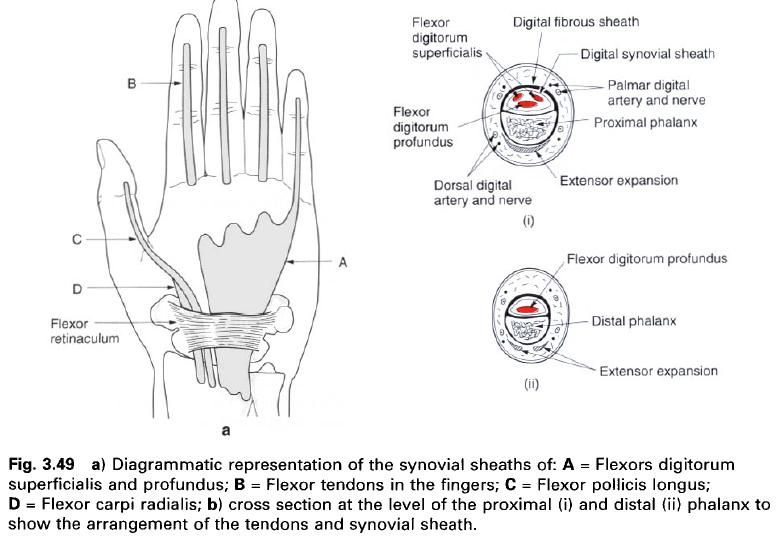
Fibro-osseous canals, retinaculae and synovial sheaths of the flexors of
the wrist and fingers
The tendons of the digital flexors are held in
close proximity to the phalanges by fibrous sheaths. These act to prevent
“bowstringing” of the tendons and ensure that their pull produces immediate
movement at the interphalangeal joints. The canals are formed by a shallow
groove on the anterior surface of the phalanges and by a fibrous sheath which
attaches to the raised lateral and medial edges of the palmar surfaces of the
proximal and middle phalanges and the palmar surface of the distal phalanx. The
canal is closed distally by attaching to the distal phalanx, but is open
proximally deep to the palmar aponeurosis. Most of the fibres of this sheath
are arranged transversely, but at the interphalangeal joints they have a
criss-cross arrangement to allow flexion to occur. All five of the fibroosseous
canals are lined with a synovial sheath which surrounds the enclosed tendons.
In the fingers, the synovial sheath surrounds the tendons of superficialis and
profundus and is connected to them by the vinculae. The sheath of the thumb
contains only the tendon of flexor pollicis longus within a synovial covering.







1 коментара:
Great post
Superficial Fascia
Постави коментар