



The synovial sternoclavicular joint provides
the only point of bony connection between the pectoral girdle and upper limb,
and the trunk. Although the joint is functionally a ball and socket joint, it
does not have the form of such a joint.
Articular
surfaces
The medial end of the clavicle articulates with
the clavicular notch at the superolateral angle of the sternum and the adjacent
upper medial surface of the first costal cartilage. The clavicular articular
surface tends to be larger than that on the sternum. Consequently, the medial
end of the clavicle projects above
the upper margin of the manubrium sterni.
The articular surfaces are reciprocally
concavoconvex, although they do not usually have similar radii of curvature.
The joint, therefore, is not particularly congruent. Congruence is partly
provided by an intraarticular fibrocartilaginous disc. The articular surface on
the manubrium sterni is set at approximately 45° to the perpendicular. It is
markedly concave from above downwards, and convex from behind forwards, being
covered with hyaline cartilage. The clavicular articular surface is convex
vertically and flattened or slightly concave horizontally, with the concavity
being continued over the inferior surface of the shaft for articulation with
the first rib costal cartilage. The greater horizontal articular surface of the
clavicle overlaps the sternocostal surface anteriorly and particularly
posteriorly, the whole being covered with fibrocartilage rather than hyaline cartilage.

Joint
capsule and synovial membrane
A fibrous capsule surrounds the whole joint
like a sleeve attaching to the articular margins of both the clavicle and the sternum, with its
inferior part passing between the clavicle
and the upper surface of the first costal cartilage. Except for this inferior
part, which is weak, the joint capsule is relatively strong, being strengthened
anteriorly, posteriorly and superiorly by capsular thickenings known as the
anterior and posterior sternoclavicular ligaments and the interclavicular
ligament respectively.
Because there are two separate cavities
associated with the joint(see below), there are two synovial membranes. A
relatively loose lateral membrane lines the capsule, being reflected from the
articular margin of the medial end of the clavicle
to the margins of the articular disc. Similarly, the medial membrane attaches
to the articular margins on the sternum and to the margins of the disc.
Intra-articular
structures
A complete, intra-articular, fibrocartilaginous
disc separates the joint into two synovial cavities. The disc is flat and
round, being thinner centrally, where it may occasionally be perforated and
permit communication between the two cavities, than around the periphery. It is
attached at its circumference to the joint capsule, particularly in front and
behind. More importantly, however, the disc is firmly attached superiorly and
posteriorly to the upper border of the medial end of the clavicle, and
inferiorly to the first costal cartilage near its sternal end. Consequently, as
well as providing some cushioning between the articular surfaces, from forces
transmitted from the upper limb, and compensating for incongruity of the joint
surfaces, the disc also has an important ligamentous action. Although mainly
fibrocartilaginous, it is fibrous or ligamentous at its circumference, and
holds the medial end of the clavicle
against the sternum. It prevents the clavicle
moving upwards and medially along the sloping sternochondral surface under the
influence of strong, thrusting forces transmitted from the limb, or when the clavicle is depressed as by a heavy
weight carried in the hand.
Ligaments
The joint capsule is strengthened anteriorly,
posteriorly and superiorly by the anterior and posterior sternoclavicular
ligaments and the interclavicular ligament respectively. In addition, an
accessory ligament, the costoclavicular ligament, binds the clavicle
to the first costal cartilage just lateral to the joint.
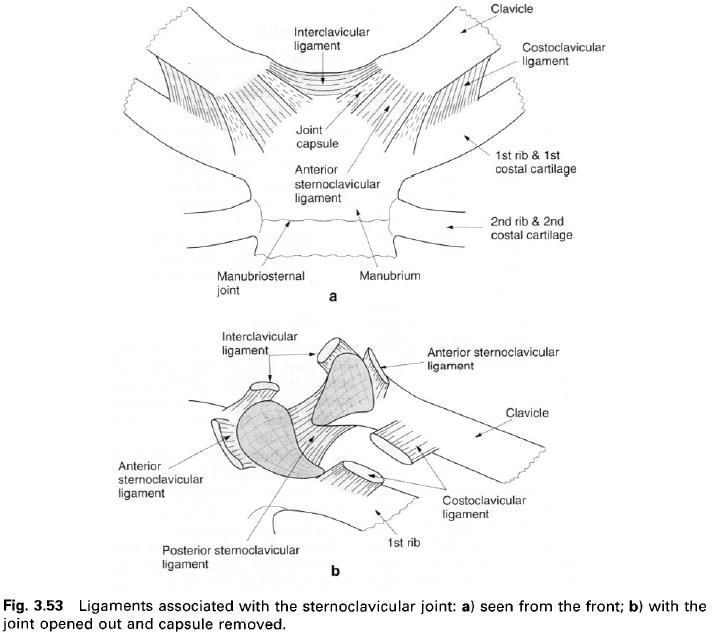
Anterior
sternoclavicular ligament
The anterior sternoclavicular ligament is a
strong, broad band of fibres attaching above to the superior and anterior parts
of the medial end of the clavicle,
passing obliquely downwards and medially to the front of the upper part of the
manubrium sterni. It is reinforced by the tendinous origin of sternomastoid.
Posterior
sternoclavicular ligament
The posterior sternoclavicular ligament,
although not as strong as the anterior ligament, is also a broad band running
obliquely downwards and medially. Laterally it attaches to the superior and
posterior parts of the medial end of the
clavicle, while medially it is
attached to the back of the upper part of the manubrium sterni. The sternal
attachment of sternohyoid extends across, and reinforces part of, the posterior
ligament.
Interclavicular
ligament
The interclavicular ligament strengthens the
capsule superiorly, and is formed by fibres attaching to the upper aspect of
the sternal end of one clavicle passing across the jugular notch to join
similar fibres from the opposite side. Some of these fibres attach to the floor
of the jugular notch.
Costoclavicular
ligament
The extracapsular costoclavicular ligament is
an extremely strong, short, dense band of fibres. It is attached to the upper
surface of the first costal cartilage near its lateral end, and to a roughened
area on the posterior aspect of the inferior surface of the medial end of the clavicle. The ligament is in two
laminae, usually separated by a bursa, which are attached to the anterior and
posterior lips of the clavicular rhomboid impression. The anterior fibres run
upwards and laterally, while those of the posterior lamina run upwards and
medially; thus the fibres have a cruciate arrangement. The direction of fibres
in the two laminae is the same as those in the external and internal
intercostal muscles respectively.
The costoclavicular ligament essentially limits
elevation of the clavicle; however,
it is also active in preventing excessive anterior or posterior movements of
the medial end of the clavicle. Its
position and strength compensate for the weakness of the adjacent inferior part
of the joint capsule.
Blood
and nerve supply
The arterial supply of the sternoclavicular
joint is from branches of the internal thoracic artery, the superior thoracic
branch of the axillary artery, the clavicular branch of the thoracoacromial
trunk, and the suprascapular artery. Venous drainage is to the axillary and
external jugular veins. Lymphatics from the joint pass to the lower deep
cervical group of nodes, sometimes called the supraclavicular nodes, and thence
to the jugular trunk. A few lymphatics may pass to the apical group of axillary
nodes.
The nerve supply of the joint is by twigs from
the medial supraclavicular nerve(C3, 4) and the nerve to subclavius(C5 and 6).
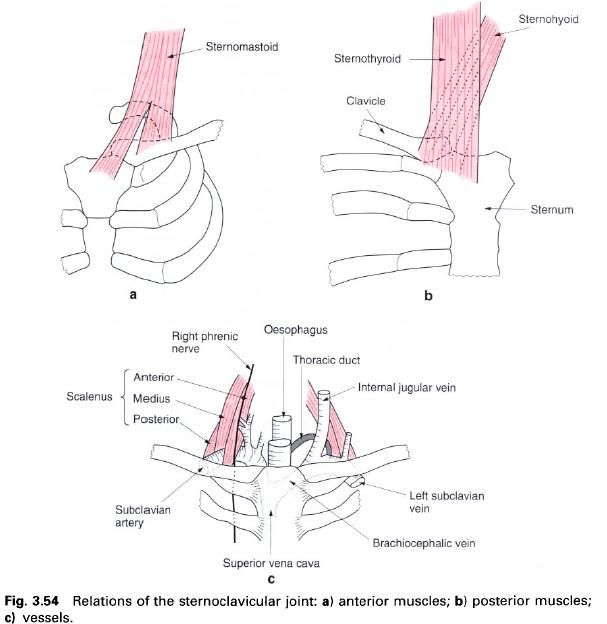
Relations
Overlying the joint anteriorly is the tendinous
attachment of the sternal head of sternomastoid. Posteriorly, the
sternoclavicular joint is separated from the brachiocephalic vein and common
carotid artery on the left and the brachiocephalic trunk, sternohyoid and
sternothyroid muscles on the right. The superior vena cava is formed on the
right hand side, by the union of the two brachiocephalic veins, just below the
joint at the lower border of the first costal cartilage.
On the right hand side, both the phrenic and
vagus nerves lie lateral to the sternoclavicular joint as they enter the thorax
from the neck. However, on the left hand side, the vagus may pass behind the
joint as it descends between the common carotid and subclavian arteries.
Stability
The shape of the articular surfaces and the
surrounding musculature provide only a limited amount of security for the
joint. The stability of the sternoclavicular joint is primarily dependent on
the strength and integrity of its ligaments, particularly the costoclavicular
ligament. Unfortunately, when dislocation of the joint takes place it is liable
to occur.
Movements
Although the articular surfaces do not conform
at those of a ball and socket joint, the sternoclavicular joint nevertheless
has three degrees of freedom of movement, that is elevation and depression,
protraction and retraction, and axial rotation. The fulcrum of these movements,
except axial rotation, is not at the joint centre but through the
costoclavicular ligament. Consequently,
the movements of elevation and depression, and protraction and retraction
involve a gliding between the clavicle and the intra-articular disc, and
between the disc and sternum.
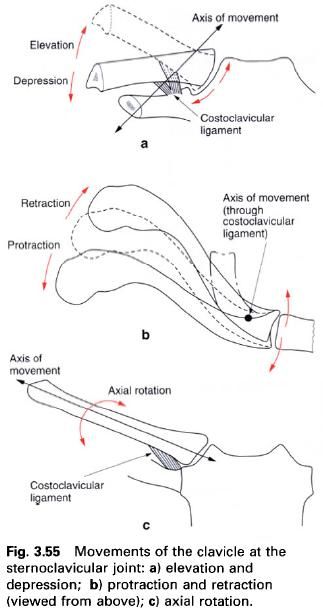
Elevation
and depression
The axis of rotation for elevation and depression
runs horizontally and slightly obliquely, anterolaterally through the
costoclavicular ligament. Some authorities have suggested that two axes of
rotation can be identified for elevation and depression, one for the gliding of
the clavicle with respect to the
disc, and the other for gliding of the disc against the sternum. Nevertheless,
functionally the combined axis of movement runs through the costoclavicular
ligament.
Because the axis of movement is somewhat
removed from the joint centre, as the lateral end of the clavicle moves, so its medial end moves in the opposite direction.
Consequently, elevation of the lateral end of the clavicle causes the medial end to move downwards and laterally. The
range of movement of the lateral end of the clavicle
is approximately 10cm of elevation and 3cm of depression, giving a total
angular range of movement of some 60°. Elevation is limited by tension in the
costoclavicular ligament and by tone in the subclavius
muscle. Depression of the clavicle,
in which the medial end moves upwards and medially, is limited by tension in
the interclavicular ligament and by the intra-articular disc. If these two
mechanisms fail, then movement is eventually limited by contact between the clavicle and upper surface of the first
rib.
Protraction
and retraction
The axis of movement for protraction and
retraction lies in a vertical plane running obliquely, inferolaterally through
the middle part of the costoclavicular ligament. Again the two ends of the clavicle move in opposite directions
because of the position of the fulcrum about which movement takes place, so
that in protraction of the lateral end, the medial end moves back and vice
versa. In these movements, the medial end of the clavicle and the
intra-articular disc tend to move as one unit against the sternum. The range of
movement of the lateral end of the clavicle
is approximately 5cm of protraction(anterior movement) and 2cm of
retraction(posterior movement), giving a total angular range of movement of
about 35°. Movement anteriorly is limited by tension in the anterior
sternoclavicular and costoclavicular ligaments, while posterior movement is
limited by the posterior sternoclavicular and costoclavicular ligaments.
Axial
rotation
Whereas elevation, depression, protraction and
retraction of the clavicle are active
movements brought about by direct muscle action, axial rotation is entirely
passive, being produced by rotation of the scapula
and transmitted to the clavicle by
the coracoclavicular ligament. Pure axial rotation of the clavicle is not possible in the living subject; it always
accompanies movements in other planes. The axis about which rotation occurs
passes through the centre of the articular surfaces.
The range of movement is small when the clavicle is in the frontal plane, but
increases considerably when the lateral end of the clavicle is carried backwards. The degree of axial rotation
possible is between 20° and 40° depending on the position of the clavicle.
That there should be any axial rotation possible
at the sternoclavicular joint is due to the relative incongruity of the
articular surfaces, the presence of an intra-articular disc and the relative
laxness of the capsular thickenings.
Accessory
movements
With the subject lying supine, a downward pressure
by the thumb on the medial end of the clavicle produces a posterior gliding of
the clavicle against the sternum.
Palpation
The line of the sternoclavicular joint can be
easily identified through the skin and subcutaneous tissues at the medial end of
the clavicle. The projection of the
medial end of the clavicle above the
sternum can also be palpated.





0 коментара:
Постави коментар