



The following sections cover some of the
physiologica adaptations that occur with prolonged altitude exposure. These
include changes at the pulmonary, cardiovascular, and muscle tissue(cellular)
level. In general, these adaptations take longer to fully develop(several weeks
to several months) than those associated with heat acclimation(typically one to two weeks). Generally, about
three weeks are needed for full acclimatization to even moderate altitude. For
each additional 600m(1,970ft) altitude increase, another week is needed an
average. All of these beneficial effects are lost within a month of return to
sea level.
Pulmonary adaptations
One of most important adaptations to altitude
is an increase in pulmonary ventilation, both at rest and during exercise.
Within three or four days at 4,000m(13,123ft), the increased resting
ventilation rate levels off at a value about 40% higher than at sea level.
Submaximal exercise ventilatory rate also plateaus at about 50% higher but over
a longer time frame. Increases in ventilation during exercise remain elevated
at altitude and are more pronounced at higher exercise intensities.
Blood adaptations
During the first two weeks at altitude, the
number of circulating erythrocytes increase. The lack of oxygen at altitude
stimulates the renal release of EPO. Within the first 3h after the athlete
arrives at a high elevation, the blood’s EPOconcentration increases; it then continues to increase for two to three days.
Although blood EPO concentrations
return to baseline levels about a month, the polycythemia(increased red blood cells) may be evident for three
months or more. After a person lives at 4,000m(13,123ft) for about six months,
his or her total blood volume(composed mainly of the red cell volume and the
plasma volume) increases by about 10% not only as a result of the altitude –
induced stimulation of eryhtrocite production but also because of plasma volume
expansion.
The percentage of total blood volume composed
of erythrocytes is reffered to as the hematocrit. Residents in the central
Andes of Peru(4,540m, or 14,895ft) have an average hematocrit of sea-level
residents, which is only 45% to 48%. However, during six weeks of exposure to
the Peruvian altitude, sea-level residents have shown remarkable increases in
their hematocrit levels, up to an average of 59%.
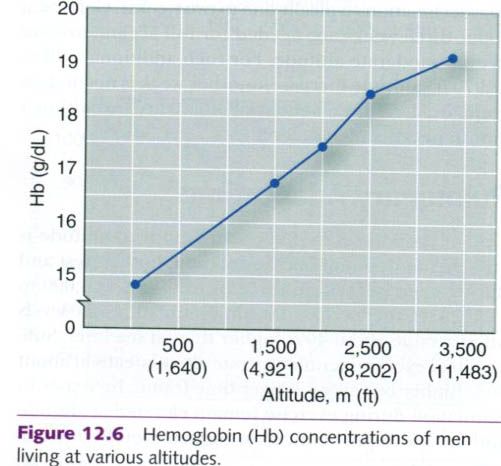
As the volume of erythrocytes increases, so
does the blood’s hemoglobin content. As noted in the figure below, blood
hemoglobin concentration needs to increase proportionately with increases in
the elevation at which people reside. The data presented are for men. For
women, however, the limited available data show a similar trend but with a
lower concentration than for men at a given altitude. These adaptations improve
the oxygen-carrying capacity of a fixed volume of blood.
The reduction in plasma volume during acute
altitude exposure reduces total blood volume, thus reducing submaximal and
maximal cardiac output. But with
acclimatization, as plasma volume increases over several weeks at altitude as
red blood cells continue to increase, maximal cardiac output increases.
However, it does not return to sea-level values. Thus, overall oxygen delivery
capacity is increased with acclimatization but not to the extent needed to
achieve sea-level VO2max
values.
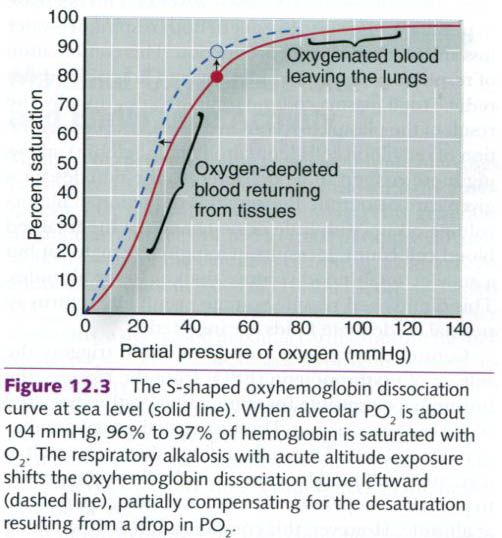
There is some debate about whether
acclimatization alters oxygen transport in the blood by changing the shape and
position of the oxyhemoglobin dissociation curve(picture below). The concentration of
2,3-diphosphoglycerate(2,3-DPG) increases in red blood cells, which shifts the
curve to the right. This would favor unloading of oxygen at the tissues(because
more oxygen would be unloading from hemoglobin at any given low arteral PO2),
but this effect opposes the loading benefit of the respiratory alkalosis, a leftward shift. The net effect of both
mechanisms is variable.
Muscle adaptations
Although few attempts have been made to study
muscle changes that occur during exposure to altitude, sufficient muscle biopsy
data exist to indicate that muscles undergo significant structural and
metabolic changes during ascent to altitude. Table below summarizes some of the
muscle adaptations that occurred over a four-to-six-week period of chronic hypoxia during expeditions to Mount
Everest and Mount
McKinley
|
Approximate
changes in muscle structure and metabolic potential during four to six weeks
of chronic hypoxia
|
||
|
Muscle
characteristic
|
Direction
of change
|
%
change
|
|
Muscle
area
|
decreased
|
12
|
|
decreased
|
20-25
|
|
|
decreased
|
20
|
|
|
Capillary
density(capillaries per mm2)
|
increased
|
15
|
|
Succinate
dehydrogenase
|
decreased
|
25
|
|
Citrate
synthase
|
decreased
|
20
|
|
Phosphorylase
|
decreased
|
30
|
|
Phosphofructokinase
|
decreased
|
50
|
The cause of the decreased muscle
cross-sectional area within the first days and weeks at altitude is not fully
understood. Prolonged exposure to high altitude frequently causes a loss of
appetite and a noticeable weight loss. During a 1992 expedition to climb Mount McKinley
Several weeks at altitudes above
2,500m(8,202ft) reduce the metabolic potential of muscle, although this may not
occur at lower elevations. Also presented in the table above, are data from
experiments performed on Mount McKinley and Mount Everest
showing that mitochondrial function and glycolytic enzyme activities of the leg
muscles(vastus lateralis and gastrocnemius) are significantly reduced after
four weeks at altitude. This suggests that, in addition to receiving less
oxygen, muscles lose some of their capacity to perform oxidative
phosphorylation and generate ATP. Unfortunately,
no muscle biopsy data have been obtained from long-term residents at high
altitudes to determine whether those individuals experience any muscular
adaptations as a consequence of lifelong residence at these elevations.












0 коментара:
Постави коментар