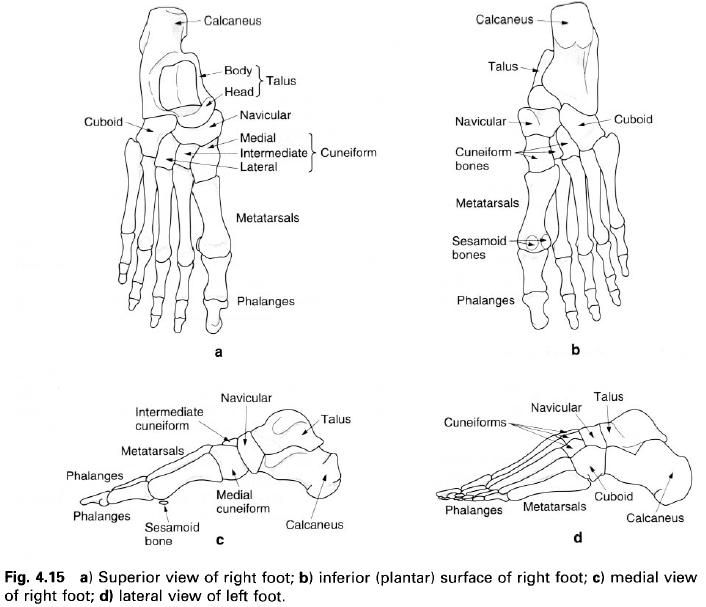
THE METATARSALS
There are five metatarsal bones in each foot,
the most medial of which is by far the stoutest, although it is also the
shortest. The second metatarsal is the longest, whilst the fifth can be
recognized by the large tubercle which projects backwards and laterally from
its base. All five metatarsals have certain features in common: a shaft, with a
head distally, and a base at the proximal end. The bases articulate with the
tarsal bones while the heads articulate with the proximal phalanx of each toe.
The base of the first metatarsal is concave
from side to side and flat from top to bottom, articulating with the anterior
surface of the medial cuneiform. Its lateral surface has a facet for
articulation with the base of the second metatarsal, whilst its inferior
surface projects downwards ending as a tuberosity. The base of the second
metatarsal articulates with the intermediate cuneiform posteriorly. Medially it
articulates with the medial cuneiform and the first metatarsal, and laterally
with the lateral cuneiform and the third metatarsal. The base of the third
metatarsal is flat and articulates with the lateral cuneiform, and on either
side with the adjacent metatarsals. It is roughened on its upper and lower
surfaces. The fourth and fifth metatarsal bases articulate with the anterior
surface of the cuboid. The fourth has a small facet on either side for
articulation with the adjacent metatarsals, whereas the fifth base is more
expanded, having a large tubercle on its lateral side. The upper and lower
surfaces of each are roughened.
All the shafts are more or less cylindrical in
form, the first being the thickest and the second usually being the thinnest.
All, however, become narrower as they pass forward towards their heads.
The heads are smooth, convex from above
downwards as well as from side to side. On either side, just behind the head,
is a tubercle in front of which is a small depression for the attachment of
ligaments. The superior non-articular surface is roughened, while the inferior
surface is marked by a groove passing forwards, which gives passage to the long
and short flexor tendons. The head of the first metatarsal is large and wide
forming the ball of the great toe. It articulates with the base of the first
phalanx and two sesamoid bones. The plantar surface of this bone is grooved, on
each side of a prominent central ridge, by the sesamoid bones in the tendons of
the short muscles which pass inferior to it.
THE PHALANGES
There are two phalanges in the great toe and
three in each of the other toes. They are miniature long bones having a shaft
and two extremities and with certain features in common. Each of the bases of
the proximal phalanges has a proximal surface which is smooth and concave for
articulation with the head of its metatarsal. The remaining phalanges have a
proximal surface divided into two by a vertical ridge. Each bone is flattened
on its plantar surface and rounded on its dorsum. The head of each bone, except
the terminal phalanges, is divided into two condyles by a vertical groove
giving it a pulley shape. The articular surface tends to be more extensive on
the plantar surface of the head where it joins the flattened surface of the
shaft. The sides of the heads are roughened, being marked by a small tubercle
at the centre.
The head of each distal phalanx is flattened on
its dorsum and has no articular area. This surface is, of course, the nail-bed.
Ossification
of the bones of the foot
Each tarsal bone ossifies from a primary centre
which appears in the cartilaginous precursor. The calcaneus is the only tarsal
bone to have a secondary centre. The primary centres for the calcaneus and
talus appear before birth in the sixth and eighth months in utero respectively.
That for the cuboid appears at nine months in utero and may therefore be
present at birth; if not, it appears soon afterwards. The centres of
ossification for the remaining bones appear as follows: at the end of the first
year for the lateral cuneiform and navicular, and during the fourth year for the
intermediate cuneiform. Ossification of these bones is completed shortly after
puberty.
The secondary centre for the calcaneus appears
at about 9 years in its posterior end and extends to include the medial and
lateral processes. Fusion occurs between 15 and 20 years. Occassionally, the
lateral tubercle may ossify separately.
Because the ossification centres for the
calcaneus, talus and cuboid are usually present before birth, they can be used
to assess the skeletal maturity of a new-born child. They may be used in
conjunction with the secondary centres in the distal end of the femur and in
the proximal end of the tibia.
The
metatarsals
A primary centre appears in the body of each
metatarsal at 9 weeks in utero, so that at birth they are well ossified.
Secondary centres appear in the base of the first metatarsal and in the heads
of the remaining metatarsals during the second and third years, with the medial
ones appearing earlier. Fusion of the epiphyses with the bodies occurs between
15 and 18 years. In the lateral metatarsals, the epiphyses may occasionally be
found in the bases instead of the heads.
The
phalanges
The primary centres for the distal and proximal
phalanges appear during the fourth month in utero, with the distal ones
appearing first. The primary centre for the middle phalanx appears between 6
months and birth. Secondary centres for the bases of all phalanges appear
during the second and third years and fuse with the bodies between 15 and 20
years.
It is interesting to note that the first
metatarsal has an ossification pattern similar to that of the phalanges. It
could be argued that instead of the middle phalanx being missing in the great
toe it is the metatarsal, so that what we now refer to as the first metatarsal
is in fact an enlarged proximal phalanx.
Palpation
of the bones of the foot
Posteriorly, the calcaneus can clearly be
identified being subcutaneous on its lateral, posterior and medial aspects. The
inferior surface is covered with thick plantar fascia, but the medial and lateral
tubercles are identifiable on deep palpation posteriorly. Medially, 1cm below
the tip of the medial malleolus, the sustentaculum tali appears as a horizontal
ridge, whilst on the lateral aspect, the
peroneal tubercle lies approximately 2cm below and in front of the tip of the
lateral malleolus, with the lateral tubercle of the calcaneus( for the
attachment of the calcaneofibular ligament) a little behind and above.
The head and neck of the talus can be grasped
between the finger and thumb in the two hollows just anteroinferior to the
malleoli, the tubercle of the navicular forming a clear landmark anterior to
the medial hollow. Midway along the lateral border of the foot, the base of the
fifth metatarsal, with its tubercle pointing posteriorly, is prominent. The
bases of the fourth to the first metatarsals can be identified crossing the
dorsum of the foot, the base of the first being 1cm anterior to the tubercle of
the navicular, the medial cuneiform being interposed.
The shafts and heads of the metatarsals can be
readily palpated on the dorsum of the foot with the bases proximally and heads
towards the toes. If the toes are extended, the heads of the metatarsals,
especially the first, will become palpable under the forefoot. The heads are a
little less obvious on the dorsum of the foot when the metatarsophalangeal
joints are flexed.
The proximal phalanx of each toe is easily
recognized, being the longest of the three; the rest are hidden to a certain
extent by the pulp of the toe.