



Gluteus medius
Gluteus minimus
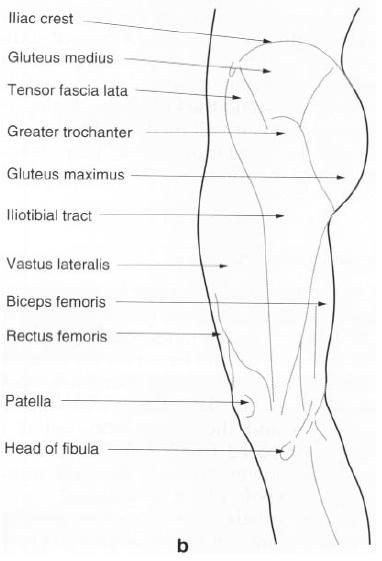
Tensor fascia latae
Gluteus medius
Gluteus medius is situated on the lateral and
upper part of the buttock, just below the iliac crest. It must be considered to
be a close companion of gluteus maximus
and is in fact overlapped by this muscle from the back. It is fan-shaped,
having its broad part above and its tendon below. It fills the space between
the iliac crest and the greater trochanter of the femur.
Its upper attachment is to the gluteal, or lateral surface of the ilium between the posterior and anterior
gluteal lines. This area is quite extensive reaching to the iliac crest above
and almost as far as the sciatic notch below. The muscle is covered with a
strong layer of fascia from the deep surface to which it has a firm attachment.
It shares the posterior part of this fascia with gluteus maximus.
The posterior fibres pass downwards and
forwards, the middle fibres pass straight downwards and the anterior fibres
pass downwards and backwards. The fibres come together and form a flattened
tendon which attaches to a roughened area, which runs downwards and forwards,
visible on the superolateral side of
the greater trochanter of the femur. The tendon is separated from the
trochanter by a bursa, whose position is given by a smooth area on the
trochanter in front of the attachment of the tendon.
Nerve
supply
Gluteus medius is supplied by the superior gluteal nerve, root value L4,
5, S1. The skin covering the muscle is mainly supplied from L1, 2.
Action
With the pelvis fixed, gluteus medius will pull
the greater trochanter of the femur upwards.
However, as the fulcrum of the movement is at the hip joint, this will cause
the femoral shaft to move laterally, this is termed abduction.
If the lower attachment of the muscle is fixed
it will pull down the wing of the ilium, producing a downward tilting of the
pelvis to the same side and, of course, a raising of the pelvis on the opposite
side. In additioin, the anterior fibres of gluteus medius acting from a fixed
pelvis will help with medial rotation of the femur. Acting with the femur fixed,
these fibres rotate the opposite side of the pelvis forward.
Functional
activity
Gluteus medius plays a vital role in walking,
running and when bearing weight on one limb. When the opposite limb is taken
off the ground the pelvis on that side would tend to drop through loss of
support from below. Gluteus medius on the supporting side works very hard to
maintain, or even raise a little, the opposite side of the pelvis, allowing the
raised limb to be brought forward for the next step. If the muscle is paralysed
the pelvis drops on the opposite side during this manoeuvre.
In walking or running, not only is gluteus
medius important for support, but with the help of other muscles, such as
gluteus minimus and tensor fascia lata, it produces a rotation of the hip
joint. This time with the femur the
more fixed point, it controls the pelvic rotation on the same side.
If the muscle is unable to work efficiently due
to paralysis or poor mechanics of the hip joint, the pelvis will drop on the
opposite side. This is reffered to as a Trendelburg sign. Walking in the case
is awkward and difficult, and running virtually impossible.
Palpation
Find the middle of the iliac crest, which is
directly above the greater trochanter of the femur. About two fingers’ breadth below this region is the bulk of
the muscle. Now stand alternately on one limb and then the other; you will feel
the muscle become hard as the weight is borne on the same limb. Place the
fingers of the other hand on the
opposite side; walk slowly down the room. You will feel the two muscles coming
into action alternately.
A patient with a Trendelburg gait, either on
one or both sides, compensates for the lack of support of the swing limb by
throwing the trunk over the supporting limb so that the weight is balanced over
the hip, thus giving time to swing
the limb through.

Gluteus minimus
Although this is the smallest of the gluteal
muscles it takes the largest attachment from the gluteal surface of the ilium.
It is triangular in shape, being wide at the top and narrowing to a tendon
below.
Its upper attachment is from the gluteal surface of the ilium in front of the anterior and above
the inferior gluteal lines, reaching as far forward as the anterior border of
the ilium in front and almost to the sciatic notch behind. Its fibres pass
downwards, backwards and slightly laterally forming a tendon which attaches to
a small depression on the anterosuperior
aspect of the greater trochanter of
the femur.
Nerve
supply
Gluteus minimus is supplied by the superior gluteal nerve, root value L4,
5, S1. The skin overlying the muscle is mainly supplied by L1.
Action
If the upper attachment of the muscle is fixed,
contraction of its anterior fibres will medially rotate the femur. This is because the femoral
attachment lies lateral to the fulcrum of the movement, the hip joint. If the
lower attachment is fixed, the muscle will raise the opposite side of the
pelvis in a similar way to gluteus medius. It will also, by pulling the front
of the ilium outwards, swing the opposite side of the pelvis forwards.
Functional
activity
This muscle appears to play its most important
role in the support and control of pelvic movements. It is a well-developed and
powerful muscle, using its power to a maximum in walking and running when the
opposite limb is off the ground. As the limb is swung forward, the pelvis on
the same side is also swung forward. This uses the hip of the weight-bearing limb as the fulcrum of the movement, with
gluteus medius and minimus both supporting the pelvis and swinging it forward
on the opposite side.
Palpation
Find the anterior superior iliac spine at the
front of the iliac crest. Allow the pads of your finger to slip downwards and
backwards towards the greater trochanter of the femur. Within two fingers’ breadth you will be on the muscle bulk.
Now rotate the lower limb medially and you will feel the muscle belly
contracting hard. Do the same on the opposite side of the body and then begin
to walk forward. You will feel the muscles contracting alternately, as each
limb becomes weight-bearing.
Tensor fascia latae
Tensor fascia latae is situated anterolateral
to the hip joint and superficial to gluteus minimus. It attaches above to the anterior part of the outer lip of the iliac
crest, between and including the iliac
tubercle and the anterior superior
iliac spine, the area of gluteal
surface just below it, the fascia between it and gluteus minimus and that covering
its superficial surface. Inferiorly, it attaches between the two layers of the
iliotibial tract, below the level of the greater trochanter.
Nerve
supply
Tensor fascia latae is supplied by the superior gluteal nerve, root value L4,
5, with the skin overlying the muscle supplied by L1.
Action
This muscle overlies gluteus minimus and helps
in flexion, abduction and medial rotation of the hip joint. It also straightens
out the backward pull of gluteus maximus
on the iliotibial tract.
Acting with the superficial fibres of gluteus maximus it will tighten the
iliotibial tract, and through its attachment to the lateral condyle of the tibia, will extend the knee joint.
Acting with gluteus minimus it will medially rotate the hip joint and its
posterior fibres may help in abduction of the thigh.
Functional
activity
Due to the fact that this muscle, together with
gluteus maximus, links the pelvis with the tibia it will help to steady and control the movements of the pelvis and femur on the tibia when the limb is weight-bearing.
Tensor fascia latae produces strong medial rotation when the hip is in extension and the lower limb,
pelvis and trunk are prepared to take the thrust relayed through the lower limb
by the calf muscles during the “toe-off” phase of walking.
When the quadriceps femoris is paralysed,
tensor fascia lata can be developed to produce sufficient extension of the knee
to enable the patient to walk, but its action is only weak and limited in
range.
Palpation
Place the fingers half way between the anterior
superior iliac spine and the greater trochanter of the femur. When the lower limb is medially rotated, the muscle can be
felt to contract powerfully. If the weight is taken on the limb and the pelvis is rotated to the same side, a
similar contraction of the muscle will be observed.






0 коментара:
Постави коментар