



- Strength
- Cardiovascular and
respiratory function
- Metabolic function,
including aerobic capacity, running economy, and anaerobic capacity
Strength
Strength improves as muscle mass increases with
age. Peak strength usually is attained by age 20 in women and between ages 20
and 30 in men. The hormonal changes that accompany puberty lead to marked
increases in strength in pubescent males because of the increased muscle mass
noted before. The extent of development and the performance capacity of muscle
also depend on the relative maturation of the nervous system. High levels of
strength, power, and skill are impossible if the child has not reached neural
maturity. Myelination of many motor nerves is incomplete until sexual maturity,
so the neural control of muscle function is limited before that time.
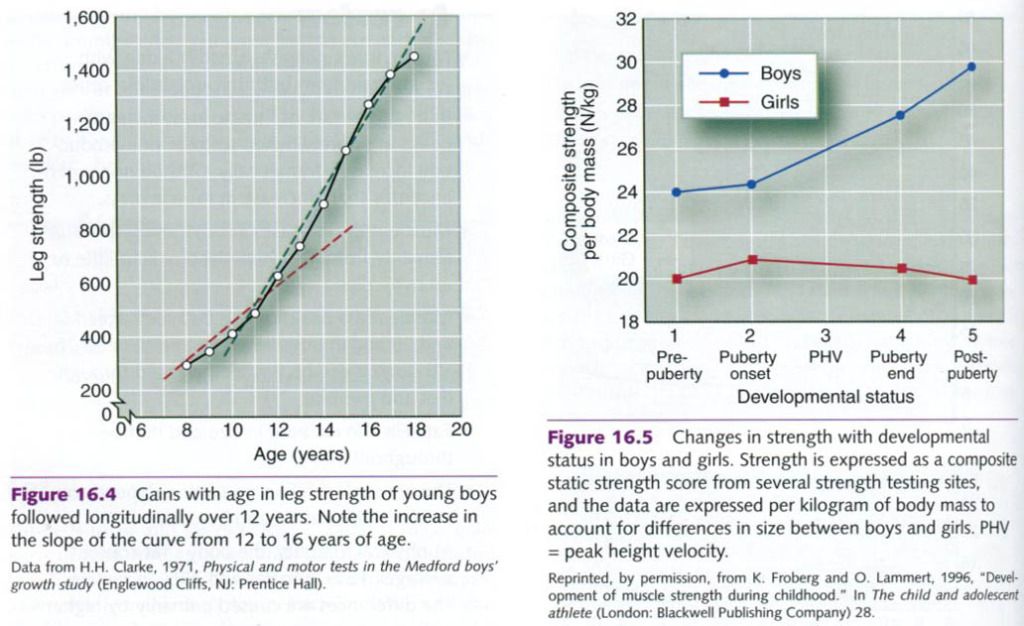
Figure below illustrates changes in leg
strength in a group of boys from the Medford Boys’ Growth Study. The boys were
followed longitudinally from age 7 to 18. The rate of strength gain(slope of
line) increased noticeably around age 12, the typical age for onset of puberty.
Similar longitudinal data for girls over this same age span are not available.
Cross-sectional data, however, indicate that girls experience a more gradual
and linear increase in strength and do not exhibit a marked change in their
rate of strength gain with puberty, also illustrated on the picture below.
Cardiovascular and respiratory function
Cardiovascular function undergoes considerable
change as children grow and age. Let’s consider some of these changes during
submaximal and maximal exercise.
Rest and submaximal exercise
Blood pressure at rest and during submaximal
levels of exercise is lower in children than in adults but progressively
increases to adult values during the late teen years. Blood pressure is also
directly related to body size. Larger people generally have higher blood
pressures, so size is at least partially responsible for children’s lower blood pressure values. In addition,
blood flow to active muscles during exercise in children can be greater for a
given volume of muscle than in adults because children have less peripheral
resistance.
Recall that cardiac output is the product of heart rate
and stroke volume. A child’s smaller
heart size and total blood volume result in a lower stroke volume, both at rest
and during exercise, than in adult. In an attempt to compensate for this, the
child’s heart rate response to a given rate of submaximal work(such as on a
cycle ergometer), where the absolute oxygen requirement is the same, is higher
than an adult’s. As the child ages, heart size and blood volume increase along with body size. Consequently, stroke volume also increases, as body
size increases, for the same absolute rate of work.
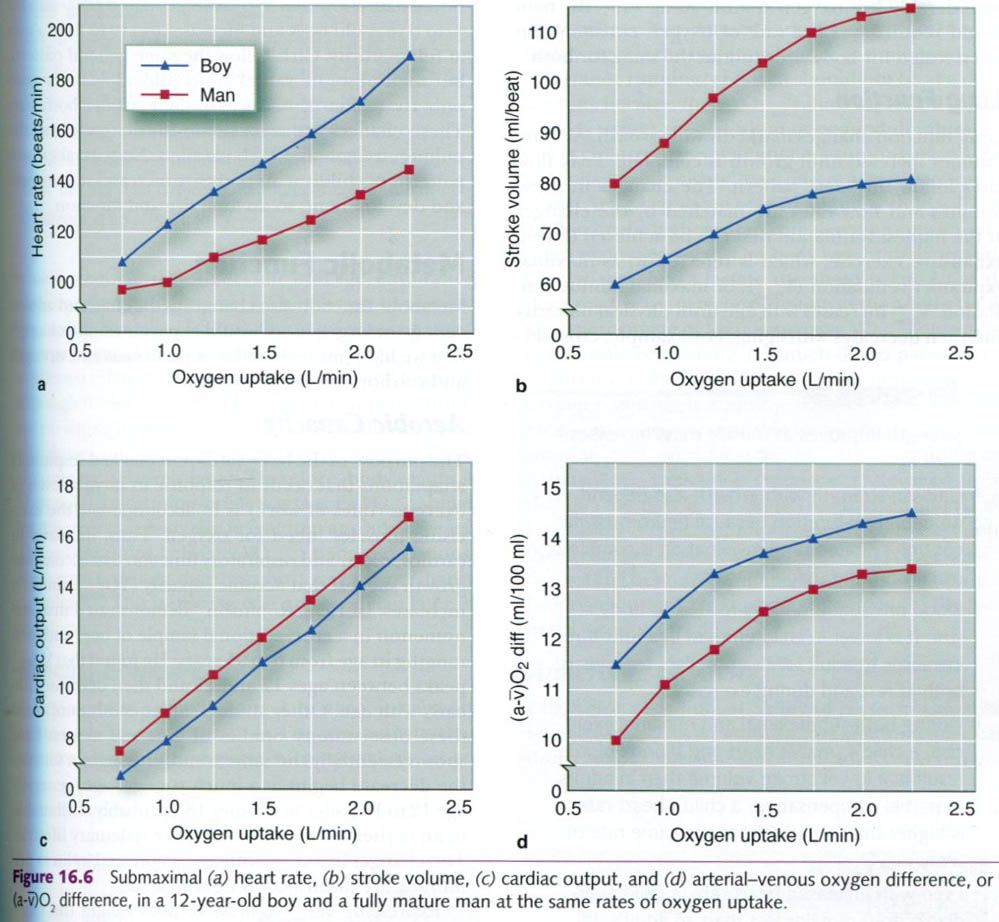
However, a child’s higher submaximal heart rate
cannot completely compensate for the lower stroke volume. Because of this, the child’s cardiac output is also somewhat lower than the adult’s for a given absolute rate of
work or a given oxygen consumption. To maintain adequate oxygen uptake during
these submaximal levels of work, the
child’s arterial-mixed venous oxygen difference, or (a-ṽ)O2 difference, increases to further compensate for
the lower stroke volume. The increase in (a-ṽ)O2 difference is most likely attributable to increased blood flow to the
active muscles – a greater percentage of the cardiac output goes to the active
muscles. These submaximal relationships are illustrated in the figure below, in
which the responses of a 12-year-old boy are compared to those of a fully
mature man.
Maximal exercise
Maximum heart rate(HRmax) is higher
in children than in adults but decreases linearly as children age. Children
under age 10 frequently have maximum heart rates exceeding 210 beats/min,
whereas the average 20-year-old has maximum approximately 195 beats/min. With
further aging(25-30 years and older), however, results of cross-sectional
studies suggest that maximum heart rate decreases by slightly less than 1
beat/min per year. Longitudinal studies, on the other hand, suggest that
maximum heart rate decreases only 0.5 beats/min per year. Longitudinal studies,
in which the same people are followed over time, generally provide more
accurate estimates of the true changes.
During maximal exercise, as also seen with
submaximal exercise, the child’s smaller heart and blood volume limit the
maximal stroke volume that he or she can achieve. Again, the high HRmax cannot
fully compensate for this, leaving the child with a lower maximal cardiac
output than the adult. This limits the child’s performance at high absolute
rates of work(e.g., pedaling at 100W on a cycle ergometer or trying to achieve
the same absolute VO2max)
because the child’s capacity for oxygen delivary is less than an adult’s.
However, for high relative rates of work in which the child is responsible for
moving only his or her body mass(e.g., running on a treadmill at the same speed
with no grade), this lower maximal cardiac output is not as serious as
limitation. In running, for example, a 25kg(55lb) child requires(in proportion
to body size) considerably less oxygen than a 90kg(198lb) man would require,
yet the rate of oxygen consumption when scaled for body size is about the same
for both.
Lung function
Lung function changes markedly with growth. All
lung volumes increase until growth is complete. Peak flow rates follow the same
pattern. The changes in these volumes and flow rates are matched by the changes
in the highest ventilation that can be achieved during exhaustive exercise,
which is referred to as maximal expiratory ventilation(VEmax), or
maximal minute ventilation. VEmax
increases with age until physical maturity and then decreases with aging. For
example, cross-sectional data show that VEmax averages about 40L/min
for 4-to 6-year-old and increases to 110 to 140L/min at full maturity. Girls
follow the same general pattern, but their absolute values are considerably
lower post-puberty, primarily because of their smaller body size. These changes
are associated with the growth of the pulmonary system, which parallels the
general growth patterns for children. As body size increases with growth and
development, so do lung size and function.
Metabolic function
Metabolic function also changes as the child
and adolescent grow larger, as we would expect from the changes that we have
just reviewed in muscle mass and strength and cardiorespiratory function.
Aerobic capacity
The purpose of the basic cardiovascular and
respiratory adaptations that can occur in response to varying levels of
exercise(rates of work) is to accommodate the exercising muscles’ need for
oxygen. Thus, increases in cardiovascular and respiratory function that
accompany growth suggest that aerobic capacity(VO2max) similarly increases. In 1938, Robinson
demonstrated this phenomenon in a cross-sectional sample of boys and men
ranging in age from 6 to 91 years. He found that VO2max peaks between ages 17 and 21 and then decreases
linearly with age. Other studies subsequently confirmed these observations.
Studies of girls and women have shown essentially the same trend, although in
females the decrease begins at a much younger age, generally age 12 to 15, probably
attributable to an earlier assumption of a more sedentary lifestyle. The
changes in VO2max with
age, expressed in liters per minute, are illustrated in the figure a below.
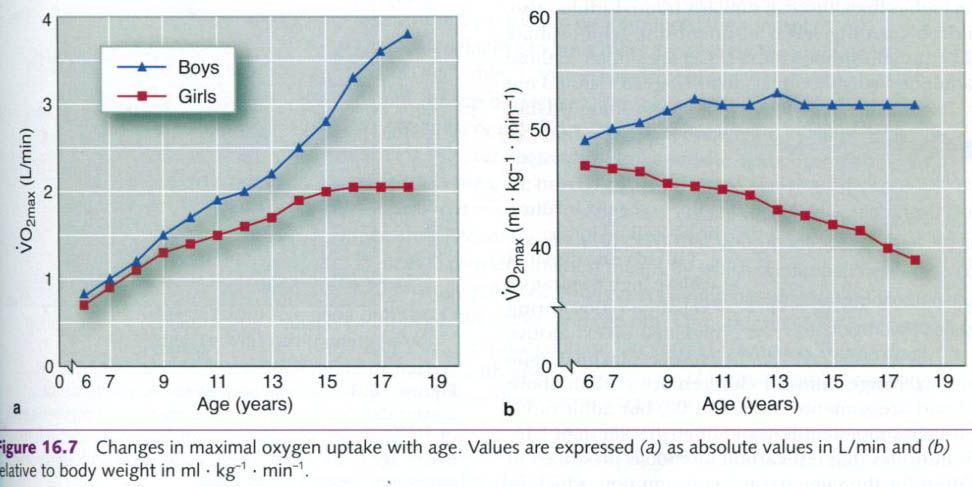
Expressing VO2maxrelative to body weight( ml x kg-1 x min-1) provides
a considerably different picture, as shown in the figure b. Values change
little in boys from age 6 to young adulthood. For girls, however, little change
occurs from age 6 to 13; but after age 13, aerobic capacities show a gradual
decrease. Although these observations are of general interest, they might not
accurately reflect the development of the cardiorespiratory system as children
grow and their physical activity levels change. Several concerns have been
raised about the validity of using body weight to account for changes in the
size of the cardiorespiratory and metabolic systems, as when one is dividing
absolute values by body weight, for example, VO2 per kilogram.
Arguments against using body weight to scale VO2max for differences in
size include the following: First, although VO2max values expressed relative to body weight remain relatively stable or decline
with age, endurance performance steadily improves. The average 14-year-old boy
can run the mile(1.6km) almost twice as fast as the average 5-year-old boy, yet
the two boys’ VO2max
values expressed relative to body weight are similar. Second, although the
increases in VO2max that
accompany endurance training in children are relatively small compared with
those in adults, the performance increases in these children are relatively
large. Therefore, body weight is likely not the most appropriate way to scale VO2max values for differences
in body size in children and adolescents. The relationships between VO2max, body dimensions, and
system functions during growth are extraordinarily complex.
Running economy
How do growth-related changes in aerobic
capacity affect a child’s performance? For any activity that requires a fixed
rate of work, such as cycling on an ergometer, the child’s lower VO2max limits endurance
performance. But as noted earlier, for activities in which body weight is the
major resistance to movement, such as distance running, children should not be
at a disadvantage, because their VO2max values expressed relative to body weight are already at or near adult values.
Yet children cannot maintain a running pace as
fast as adults can because of basic differences in economy of effort. At a given speed on a treadmill, a child will
have a substantially higher submaximal oxygen consumption when expressed
relative to body weight than an adult. Even if the child’s lactate thresholdoccurred at the same relative oxygen consumption as the adult’s(at the same
percentage of their respective VO2max
values), the child would be running at a much slower pace. Also, as
children age, their legs lengthen, their muscles become stronger, and their
running skills improve. Running economy increases, and this improves their
distance-running pace, even if the children are not training and if their VO2max values don’t increase.
Rowland argues that increased stride frequency as children and adolescents grow
is the most important factor in explaining these changes in running economy. It
is also possible that scaling oxygen consumption to body weight is
inappropriate during growth and development.
Anaerobic capacity
Children have a limited ability to perform
anaerobic-type activities. This is demonstrated in several ways. Children
cannot achieve adolescent or adult concentrations of lactate in either muscle
or blood for maximal and supramaximal
rates of exercise. This suggests that children have a lower glycolitic capacity. The lower lactate
levels might reflect a lower concentration of phosphofructokinase, the key
rate-limiting enzyme of anaerobic glycolysis. Lactate dehydrogenase activity also seems to be lower in
children. However, lactate threshold,
when expressed as a percentage of VO2max,
does not appear to be a limiting factor in children because children’s lactate
thresholds are similar to, if not somewhat higher than, those of similarly
trained adults. Also, children’s resting levels of adenosine triphosphate(ATP) and phosphocreatine(PCr)
are similar to those of adults, so activities of less than 10 to 15s should
not be compromised. Thus, only
activities that tax the anaerobic glycolytic system – those from 15s to 2min in
duration – will be lower.
Children cannot achieve high respiratory
exchange ratios during maximal or exhaustive exercise. Maximal respiratory exchange ratios in children
are seldom above 1.10 and are sometimes below 1.00, but adult ratios are
usually more than 1.10 and often greater than 1.15. This indicates that less
carbon dioxide is produced in children for the same oxygen consumption, which
in turn indicates less buffering of lactate.
Anaerobic mean and peak power output, as
determined by the Wingate aerobic power test(a 30s, all-out maximal effort on a
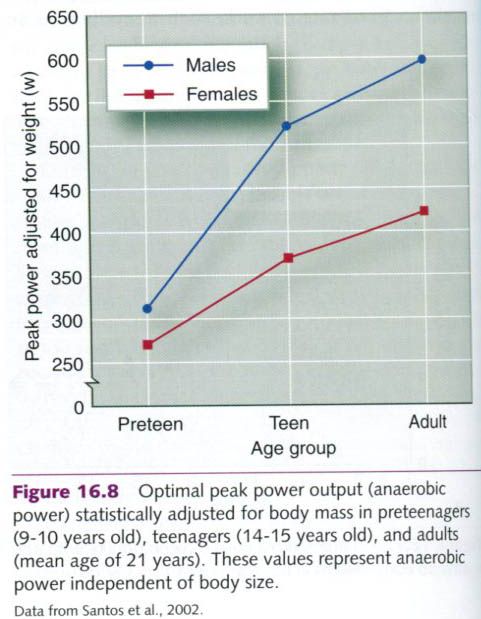
cycle ergometer), is also lower in children than in adults. Figure below
illustrates the results of a similar cycle ergometer anaerobic power test that
is potentially a better discriminator of peak power output capacity. In this
figure, peak power is statistically adjusted for body mass to account for
differences in body size when we compare values for preteenagers, teenagers,
and adults. This figure demonstrates the very low peak power outputs for
preteenagers(9-10 years of age) compared with both teenagers(14-15 years of
age) and adults(mean age of 21 years). Teenagers were much closer to the values
for adults than the preteenagers. Again, these values were adjusted for body
size, so they should accurately reflect anaerobic power.
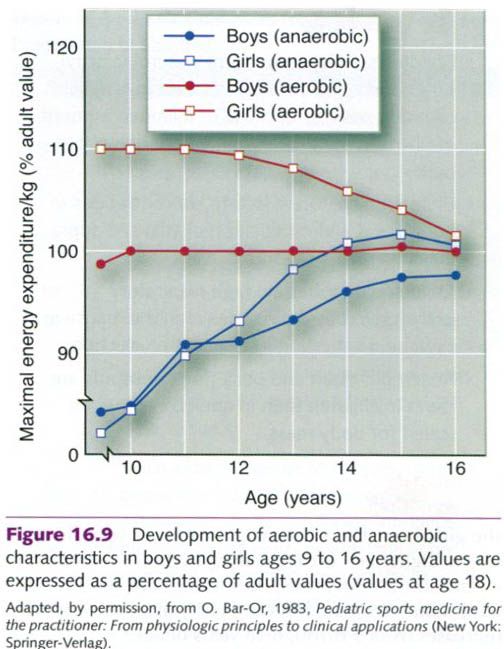
Bar-Or summarized the development of both the aerobic and anaerobic characteristics of boys and girls from ages 9 through 16,
using 18 years of age as the criterion for 100% of the adult value. The changes
with age are shown in the figure below. Aerobic power is represented by the
child’s performance on the Margaria step-running test(a field test). Maximal
energy expenditure per kilogram represents the maximal energy-generating
capacities of the aerobic and anaerobic systems, scaled to body weight
to account for body size differences with growth. Notice that aerobic fitness
remains constant for the boys but declines for the girls from 12 to 16 years. Nine-to
12-year-old girls have a higher aerobic capacity than the 18-year-old reference
adult value; thus, their values are 110% of the adult value. For both boys and
girls, anaerobic capacity increases
from 9 through 15 years of age.












0 коментара:
Постави коментар