



Relations
All of the structures entering or leaving the
hand have to cross the region of the wrist. Some of these will lie directly
against the carpal bones, others will be separated by intervening soft tissues.
The nature of the arrangement of the carpal bones, in which they form part of a
fibro-osseous canal, makes the anterior aspect of the wrist an extremely
important region.
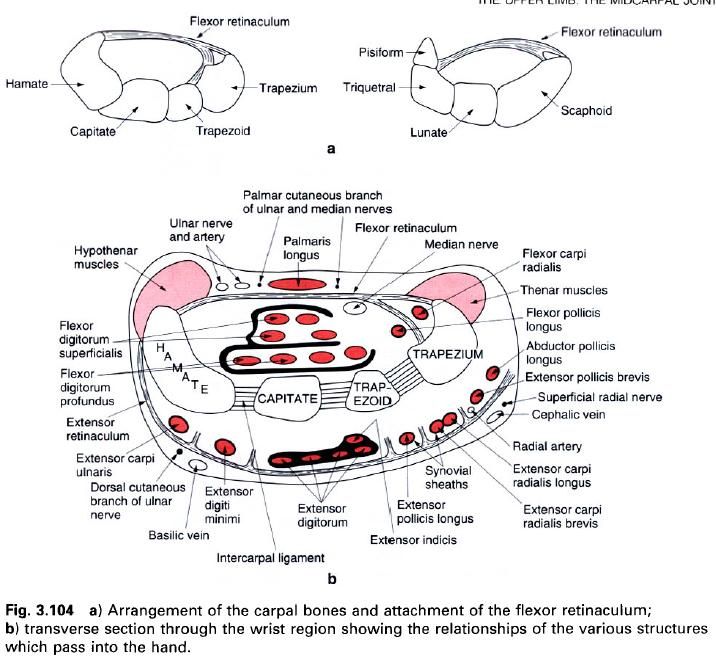
The carpal bones of each row form a transverse
arch with a palmar concavity(figure a). The principal structure maintaining the
bones in this position is the flexor retinaculum. Consequently, it is
considered by some to be an accessory ligament to the intercarpal joints. The
flexor retinaculum attaches medially to the pisiform and the hook of the
hamate, and laterally to the scaphoid tubercle and to both lips of the groove
on the trapezium so forming a small lateral compartment separate from the rest
of the canal. Passing through this lateral compartment is the tendon of flexor carpi radialis enclosed within
its own synovial sheath(b). Through the larger main part of the canal pass:
- the tendon of flexor pollicis longus most laterally, deep in the concavity of the carpal bones;
- the four tendons of flexor digitorum profundus lying side-by-side directly over the capitate;
- the four tendons of flexor digitorum superficialis overlying those of profundus, with the tendons to the third and fourth digits anterior to those for the second and fifth; the tendons of flexors digitorum superficialis and profundus being enclosed within the same synovial sheath;
- the median nerve lying lateral to the superficialis tendons(b).
Inflammation of the synovial sheaths within the
so-called carpal tunnel may lead to compression of the median nerve, and gives
rise to carpal tunnel(or median nerve)
syndrome. This leads to paraesthesia and diminution of sensory acuity in the
region of the median nerve’s sensory distribution, loss of power and limitation
of some thumb movements, together with some wasting of the thenar eminence.
Passing anterior to and blending with the flexor retinaculum is the tendon of palmaris longus. Also passing
superficial to the retinaculum on the medial side is the ulnar nerve with the
ulnar artery lateral to it. In addition, the palmar cutaneous branches of the
median and ulnar nerves, and the superficial palmar branch of the radial artery
enter the hand by crossing the
retinaculum.
On the posterior aspect of the carpal bones,
the extensor tendons pass into the hand.
They are bound down by fibrous septa passing from the deep surface of the
extensor retinaculum to ridges on the radius,
ulna and capsular tissues of the joint(upper picture b).
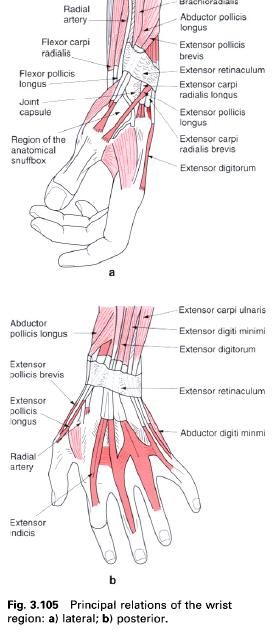
The six longitudinal compartments so formed
separate and transmit the tendons of the nine muscles of the extensor
compartment. Most laterally, over the lateral surface of the radial styloid
process and continuing over the scaphoid and trapezium, pass the tendons of abductor pollicis longus and extensor pollicis brevis within the same
synovial sheath(a). In the adjacent
compartment over the radius lateral
to the dorsal tubercle, and then over the scaphoid and the most medial part of
the trapezium and the trapezoid, run the tendons of extensor carpi radialis longus and brevis(a). In the third
compartment, in a groove on the medial side of the dorsal tubercle, is the
tendon of extensor pollicis longus(a).
However, because this tendon uses the dorsal tubercle as a pulley, it deviates
laterally towards the thumb and so crosses the scaphoid and trapezium between
the tendons of the two previous compartments. Running over the most medial part
of the dorsum of the radius, and then
over the adjacent parts of the scaphoid and lunate, and the capitate are the
four tendons of extensor digitorum, with the tendon of extensor indicis deep to them(b). All five tendons are enclosed
with a common synovial sheath. Crossing the posterior surface of the inferior
radioulnar joint, the lunate and the adjacent surfaces of the capitate and
hamate is the tendon of extensor digiti minimi(b). Finally, the tendon of extensor carpi ulnaris passes in a groove on the back of the ulna and onto the triquetral before attaching to the base of the
fifth metacarpal(b). The dorsal branch of the ulnar nerve and the terminal
branches of the superficial radial nerve cross the extensor retinaculum to
enter the dorsum of the hand on its
medial and lateral sides respectively. The other major structure to enter the hand is the radial artery, and it does
so by a convoluted route(a). In the forearm proximal to the flexor retinaculum,
the radial artery can be palpated lateral to the tendon of flexor carpi radialis. It then turns laterally to cross the radial
collateral carpal ligament, the scaphoid and trapezium, being crossed by the
tendons of abductor pollicis longus
and extensors pollicis brevis and longus before
passing into the palm of the hand
between the two heads of the first dorsal interosseus muscle. The hollowed
region between the tendons of abductor pollicis longus and extensor pollicis brevis laterally, and extensor pollicis longus medially when the thumb is extended is known as the
“anatomical snuffbox”(a). The radial artery crosses the floor of this hollow,
which is formed from proximal to distal by the radial styloid process,
scaphoid, trapezium and base of the first metacarpal; its pulsations can be
felt radially by applying firm pressure between the tendons.
Stability
Because of the attachment of the flexor
retinaculum and the numerous tendons crossing the joint both anteriorly and
posteriorly, the wrist is a relatively stable region. Nevertheless, abnormal
stresses applied to it may result in dislocation or fracture.
A fall on the outstretched hand may result in a dislocation at the radiocarpal and/or
midcarpal joints, involving anterior dislocation of the lunate. Usually this
can be reduced by manipulation. Care must be taken however in not confusing a
dislocation with a Colles’ fracture. A fall on the hand is more likely to result in the force being transmitted
through the trapezium and trapezoid to the scaphoid, which tends to fracture
across its waist. Persistent pain on applying pressure in the anatomical
snuffbox is characteristic of scaphoid fracture. Care should be taken when
setting the fracture that the two fragments are aligned and in contact,
otherwise non-union and/or a vascular necrosis may result if viable blood
vessels reach only one of the fragments. (The blood supply to the scaphoid is
from distal to proximal.)
Movements
The movements which occur at the radiocarpal
and midcarpal joints take place at the same time. The total range of flexion
and extension is therefore 85° in each direction. Flexion is limited by tension
in the extensor tendons and is greatly reduced if the fingers are fully flexed.
The main muscles providing flexion are the flexors carpi radialis and ulnaris. The
main muscles producing extension are the extensors carpi ulnaris and radialis longus
and brevis. Radiographic film shows
that flexion and extension movements at the wrist occur about a single
transverse axis through the head of the capitate.
The total range of abduction and adduction
which occurs at the wrist is also the sum of the ranges possible at the
radiocarpal and midcarpal joints. Consequently, abduction has a range of 15°
and adduction a range of 45°. The movements occur about a single anteroposterior
axis passing through the head of the capitate slightly more distal to the axis
for flexion and extension. Abduction is more limited than adduction primarily
because the radial styloid process projects further distally than the ulnar
styloid process. Abduction is brought about by flexor carpi radialis and extensors carpi radialis longus and brevis,
while adduction is achieved by flexor
and extensor carpi ulnaris.

Biomechanics
The lines of action of the muscles of the wrist
are always oblique with respect to the axes of movement. By using only one
muscle the movement produced would not be a pure movement. For example,
contraction of flexor carpi radialis
would produce flexion and abduction at the wrist. To produce pure flexion the
unwanted abduction has to be cancelled; this is achieved by contracting flexor carpi ulnaris. Thus by combining
various forces acting in different directions any desired movement can be
produced within the complete range of motion of the joint.
The carpal flexors and extensors fix the wrist
during extension or flexion of the fingers, thereby preventing the digital
muscles from losing power and efficiency, which would occur if they also acted
on the radiocarpal and midcarpal joints. When powerful movements of the fingers
are required, both the flexors and extensors of the wrist contract
simultaneously. The importance of such actions is obvious when attempts are
made to grip strongly with the finger flexors when the wrist is already flexed.
Extending the wrist stretches these muscles so that they can now exert
considerable power. Slight extension of the wrist is the position naturally
adopted when the hand is used for
gripping: look at your own wrist when writing or picking up a mug. If the wrist
is likely to become fixed through disease, it should be secured in a position
of slight extension so that a powerful and precise grip can still be achieved.
The extrinsic finger flexors are the major
force-producing muscles during exertions of the hand. Deviation of the wrist causes these tendons to move against
the adjacent walls of the carpal tunnel. When the wrist is flexed the tendons
are supported by the flexor retinaculum, and when extended by the carpal bones.
The force between the tendons and the retinaculum may compress the median nerve
and be an important factor in carpal tunnel syndrome: such compression has been
confirmed by direct pressure measurement. As well as the median nerve being
compressed, the synovial sheaths surrounding the flexor tendons are also
compressed, both in flexion and extension. This may lead to their inflammation
and subsequent swelling, leading to further compression of the median nerve.
Taking into account wrist size, the loading of the flexor retinaculum in
flexion is 14% greater in females than in males. This may be one of the reasons
why carpal tunnel syndrome is between 2 and 10 times more prevalent in women
than men.
In some cases of limitation or absence of
movement at the wrist, often associated with persistent pain, total wrist
arthroplasty can relieve pain and improve mobility.











0 коментара:
Постави коментар