



Heart rate
Aerobic training has a major impact on heart
rate at rest, during submaximal exercise, and during the postexercise recovery
period. The effect of aerobic training on maximal heart rate is not as clear.
Resting
heart rate
The heart rate at rest can decrease markedly as
a result of endurance training. A sedentary individual with an initial resting
heart rate of 80 beats/min can decrease resting heart rate by approximately 1
beat/min with each week of aerobic training, at least for the first few weeks.
After 10 weeks of moderate endurance training, resting heart rate can decrease
from 80 to 70 beats/miin or lower. The actual mechanisms responsible for this
decrease are not entirely understood, but training appears to increase
parasympathetic activity in the heart while decreasing sympathetic activity. It
is important to recognize that several well-controlled studies with large
numbers of subjects have shown much smaller decreases in resting heart rate,
that is, fewer than 5 beats/min following up to 20 weeks of aerobic training.
Bradycardia is a clinical term indicating a
heart rate of fewer than 60 beats/min. In untrained individuals, bradycardia is
usually the result of abnormal cardiac function or a diseased heart. Therefore,
it is necessary to differentiate between training-induced bradycardia, which is
a natural response to endurance training, and pathological bradycardia, which
can be a serious cause for concern.
Submaximal
heart rate
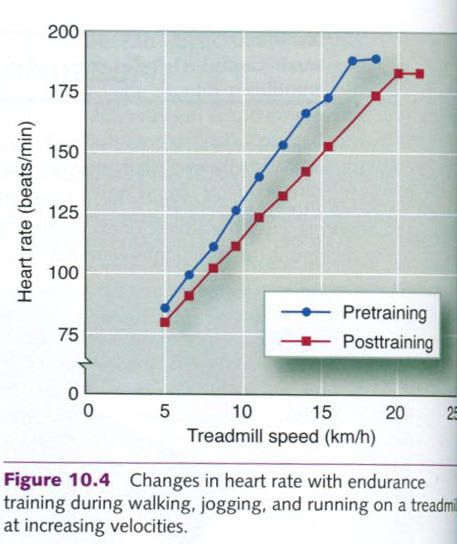
During submaximal exercise, aerobic
conditioning results in proportionally lower heart rates at a given absolute
exercise intensity. This is illustrated in figure below, which shows the heart
rate of an individual exercising on a treadmill both before and after training.
At each specified intensity, indicated here by the speed at which the subject
is walking or running, the posttraining heart rate is lower than the heart rate
before training. After a six-month endurance training program of moderate
intensity, decreases in heart rate of 10 to 30 beats/min are common at the same
absolute submaximal workload, the training-induced decrease being greater at
higher intensities.
These decreases indicate that the heart becomes
more economical through training. In carrying out its necessary functions, a
trained heart performs less work(lower heart rate, higher stroke volume) than
an unconditioned heart at the same absolute workload.
Maximum
heart rate
A person’s maximal heart rate(HRmax)
tends to be stable and typically remains relatively unchanged after endurance training.
However, several studies have suggested that for people whose untrained HRmax
values exceed 180 beats/min, HRmax might be slightly lower after
training. Also, highly conditioned endurance athletes tend to have lower HRmax
values than untrained individuals of the same age, although this is not
always the case. Athletes over 60 years old sometimes have higher HRmax
values than untrained people of the same age.
Interactions
between heart rate and stroke volume
During exercise, the product of heart rate and
stroke volume provides a cardiac output appropriate to the intensity of the
activity being performed. At maximal or near-maximal intensities, heart rate
may change to provide the optimal combination of heart rate and stroke volume
to maximize cardiac output. If heart rate is too fast, diastolic filling time
is reduced, and stroke volume might be compromised. For example, if HRmax is
180 beats/min, the heart beats three times per second. Each cardiac cycle thus
lasts for only 0.33s. Diastole is as short as 0.15s or less. This fast heart
rate allows very little time for the ventricles to fill. As a consequence,
stroke volume may decrease at high heart rates at which filling time is
compromised.
However, if the heart rate slows, the
ventricles would have longer to fill. This has been proposed as the reason
highly trained endurance athletes tend to have lower HRmax values:
their hearts have adapted to training by drastically increasing their stroke
volumes, so lower HRmax values can provide optimal cardiac output.
Which comes first? Does increased stroke volume
result in a decreased heart rate, or does a lower heart rate result in an
increased stroke volume? This question remains unanswered. In either case, the
combination of increased stroke volume and decreased heart rate is a more
efficient way for the heart to meet the metabolic demands of the body,
especially during exercise. The heart expends less energy by contracting less
often but more forcefully than it would if contraction frequency were increased.
Reciprocal changes in heart rate and stroke volume in response to training
share a common goal: to allow the heart to pump the maximal amount of
oxygenated blood at the lowest energy cost.
Heart
rate recovery
During exercise, heart rate must increase to
increase cardiac output to meet the blood flow demands of active muscles. When
the exercise bout is finished, heart rate does not instantly return to its
resting level. Instead, it remains elevated for a while, slowly returning to
its resting rate. The time it takes for heart rate to return to its resting
rate is called the heart rate recovery period.
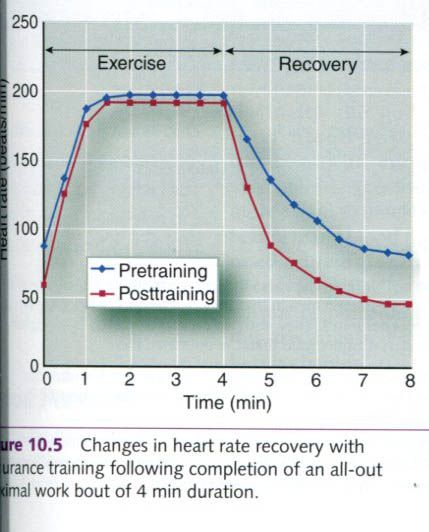
Following a period of training, as shown in the
figure below, heart rate returns to its resting level much more quickly after
exercise than it does before training. This is true after standardized
submaximal exercise as well as after maximal exercise.
Because the heart rate recovery period is
shortened after endurance training, this measurement has been proposed as an
indirect index of cardiorespiratory fitness. In general, a more fit person
recovers faster after a standardized rate of work than a less fit person, so
this measure may have some utility in field settings when more direct measures
of endurance capacity are not possible or feasible. However, factors other than
training can also affect heart rate recovery time. For example, exercise in hot
environments or at high altitudes can prolong heart rate elevation. Some people
undergo a stronger sympathetic nervous system response during exercise than
others, and this also could prolong heart rate elevation.
The heart rate recovery curve is a useful tool
for tracking a person’s progress during a training program. But because of the
potential influence of other factors, it should not be used to compare between
individuals.
Cardiac output
While stroke volume increases, heart rate
generally decreases at rest and during exercise at a given absolute intensity.
Because the magnitude of these reciprocal
changes is similar, cardiac output at rest and during submaximal exercise at a
given exercise intensity does not change much following endurance training. In
fact, cardiac output can decrease slightly. This is likely the result of an
increase in the (a-ṽ)O2
difference(reflecting greater oxygen extraction by the tissues) or a
decrease in the rate of oxygen
consumption(reflecting an increased mechanical efficiency). Generally,
cardiac output matches the oxygen consumption required for any given intensity
of effort.
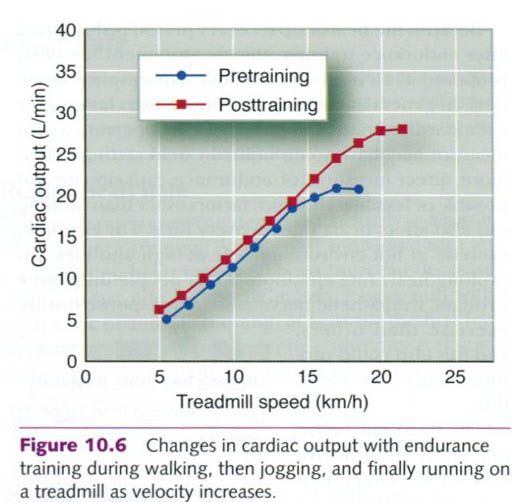
Maximal cardiac output, however, increases
considerably at maximal exercise intensity in response to aerobic training, as
seen in the figure below, and is largely responsible for the increase in VO2max.
This increase in cardiac output must result from an increase in maximal stroke
volume, because HRmax changes little, if any. Maximal cardiac output
ranges from 14 to 20L/min in untrained individuals and from 25 to 35L/min in
trained individuals, and can be 40L/min or more in highly conditioned endurance
athletes. These absolute values, however, are greatly influenced by body size.
Blood flow
Active muscles need considerably more oxygen
and nutrients than inactive ones. To meet these increased needs, more blood
must be delivered to these muscles during exercise. With endurance training,
the cardiovascular system adapts to increase blood flow to exercising muscles
to meet their higher demand for oxygen and metabolic substrates. Four
factors account for this enhanced blood flow to muscle following training:
- Increased capillarization of
trained muscles
- Greater recruitment of
existing capillaries in trained muscles
- More effective blood flow
redistribution from inactive regions
- Increased blood volume.
To permit increased blood flow, new capillaries
develop in trained muscles. This allows the blood flowing into skeletal muscle
from arterioles to more fully perfuse the active tissues. This increase in
capillaries usually is expressed as an increase in the number of capillaries
per muscle fiber, or the capillary-to-fiber
ratio. Table below illustrates the differences in capillary-to-fiber ratios
between well-trained and untrained men, both before and after exercise.
|
Muscle
fiber capillarization in well-trained and untrained men
|
||||
|
|
Capillaries
per mm2
|
Muscle
fibers per mm2
|
Capillary-to-
fiber
ratio
|
Diffusion
distance
|
|
Well
trained
|
||||
|
Preexercise
|
640
|
440
|
1.5
|
20.1
|
|
Postexercise
|
611
|
414
|
1.6
|
20.3
|
|
Untrained
|
||||
|
Preexercise
|
600
|
557
|
1.1
|
20.3
|
|
Postexercise
|
599
|
576
|
1.0
|
20.5
|
Diffusion distance is expressed as the average
half-distancce between capillaries on the cross-sectional view expressed in
micrometers.
Not all capillaries are open at any given time
in tissues, including muscle. In addition to new capillarization, existing
capillaries in trained muscles can be recruited and open to flow, which
increases blood flow to muscle fibers. The increase in new capillaries with
endurance training and increased capillary recruitment combine to increase the
cross-sectional area for exchange between the vascular system and the
metabolically active muscle fibers. Because endurance training also increases
blood volume, shifting more blood into the capillaries will not severely
compromise venous return.
A more effective redistribution of cardiac
output also can increase blood flow to the active muscles. Blood flow is
directed to the active musculature and shunted away from areas that do not need
high flow. Blood flow can increase to the more active fibers even within a
specific muscle group. Armstrong and Laughlin demonstrated that
endurance-trained rats could redistribute blood flow to their most active
tissues during exercise better untrained rats could. The researchers used
radiolabeled microspheres, radioactive particles that are injected into the
bloodstream. The distribution of these microspheres was then determined by
using a Geiger counter, which measures of the amount of radioactive material
throughout the area of interest(in this case exercising muscle). The total
blood flow to the hindlimbs did not differ between the trained and untrained
rats during exercise. However, the trained rats distributed more of their blood
to the most oxidative muscle fibers, effectively redistributing the blood flow
away from the glycolitic muscle fibers. These findings are difficult to
replicate in humans because of the technical difficulty(microspheres cannot be
used in humans) of measuring blood flow to specific muscle types, as well as
the fact that human skeletal muscle is a mosaic with mixed fiber types among
individual muscles.
Finally, the body’s total blood volume
increases with endurance training, providing more blood to meet body’s many
blood flow needs during endurance activity.
Blood pressure
Following endurance training, arterial blood
pressure is reduced at a given submaximal exercise intensity; but at maximal
exercise capacity, systolic blood pressure is increased and diastolic pressure
is decreased. Resting blood pressure in response to endurance training does not
change significantly in healthy subjects but is generally lowered in borderline
or moderately hypertensive individuals. This reduction occurs in both systolic
and diastolic blood pressure. Drops in blood pressure average approximately 6
to 7mmHg for both systolic and diastolic pressure in hypertensive subjects and
slightly less in borderline hypertensives. The mechanisms underlying this
reduction are unknown.
Although resistance-type exercise can cause
large increases in both systolic and diastolic blood pressure during lifting or
heavy weights, chronic exposure to these high pressures does not elevate
resting blood pressure. Hypertension is not common in competitive weightlifters
or in strength and power athletes. In fact, a few studies have even shown that
resistance training may lower resting systolic blood pressure. Hagberg and
coworkers followed a group of borderline-hypertensive adolescents through five
months of weight training. The subjects’ resting systolic blood pressures
decreased significantly. These reductions were somewhat greater than those
resulting from endurance training.
Blood volume
Endurance training increases blood volume, and
this effect is larger as training intensity increases. Furthermore, the effect
occurs rapidly. This increased blood volume results primarily from an increase
in plasma volume, but there is also an increase in red blood cells. The time
course for the increase of each of these is quite different.
Plasma
volume
The increase in plasma volume is thought to
result from two mechanisms. The first mechanism, which has two phases, results
in increases in the amount of plasma proteins, particularly albumin. Plasma
proteins are the major source of osmotic pressure in the vasculature. As plasma
protein concentration increases, so does osmotic pressure, and fluid is
reabsorbed from the interstitial fluid into the vasculature. During an intense
bout of exercise, proteins leave the vascular space and move into the
interstitial space. They are then returned in greater amounts through the lymph
system. It is likely that the first phase of rapid plasma volume increase is
the result of the increased plasma albumin, which is noted within the first
hour of recovery from the first training bout. In the second phase, protein
synthesis is turned on(upregulated) by repeated exercise, and new proteins are
formed. With the second mechanism, exercise increases the release of
antidiuretic hormone and aldosterone, hormones that cause increased
reabsorption of water and sodium in the kidneys, which increases blood plasma. That
increased fluid is kept in the vascular space by the oncotic pressure exerted
by the proteins. Nearly all of the
increase in blood volume during the first two weeks of training can be
explained by the increase in plasma volume.
Red
blood cells
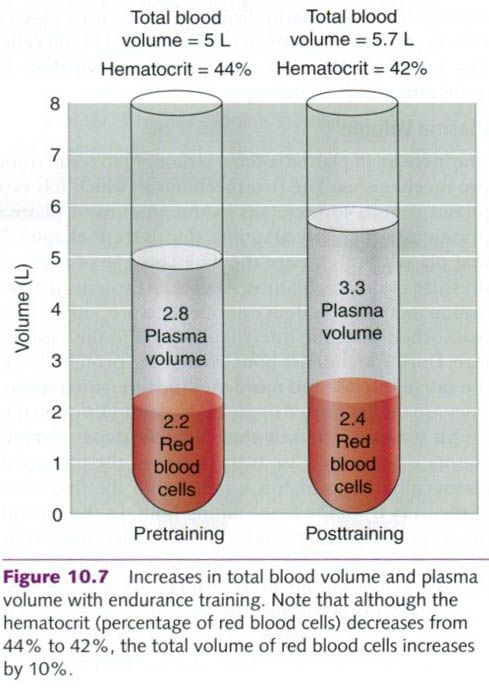
An increase in red blood cell volume with
endurance training also contributes to the overall increase in blood volume,
but this increase is an inconsistent finding. Although the actual number of red
blood cells may increase, the hematocrit – the ratio of the red blood cell
volume to the total blood volume – may actually decrease. Figure below illustrates
this apparent paradox. Notice that the hematocrit is reduced even though there
has been a slight increase in red blood cells. A trained athlete’s hematocrit
can decrease to a level where the athlete appears to be anemic on the basis of
a relatively low concentration of red cells and hemoglobin.
The increased ratio of plasma cells resulting
from a greater increase in the fluid portion reduces the blood’s viscosity, or
thickness. Reduced viscosity may facilitate blood movement through the blood
vessels, particularly through the smallest vessels such as the capillaries. One
of the physiological benefits of decreasing blood viscosity is that it enhances
oxygen delivery to the active muscle mass.
Both the total amount(absolute values) of
hemoglobin and the total number of red blood cells are typically elevated in
highly trained athletes, although these values relative to total blood volume
are below normal. This ensures that the blood has more than ample
oxygen-carrying capacity. The turnover rate of red blood cells also may be
higher with intense training.








1 коментара:
Thật quá cần thiết vì những chia sẻ của bạn, mình cho rằng là sẽ nhiều người khác cần đến những ý kiến bạn vừa mới chia sẻ
Tôi cũng đóng góp 1 chút những kinh nghiệm tại link sau đây: đồ tập thể dục
Постави коментар