



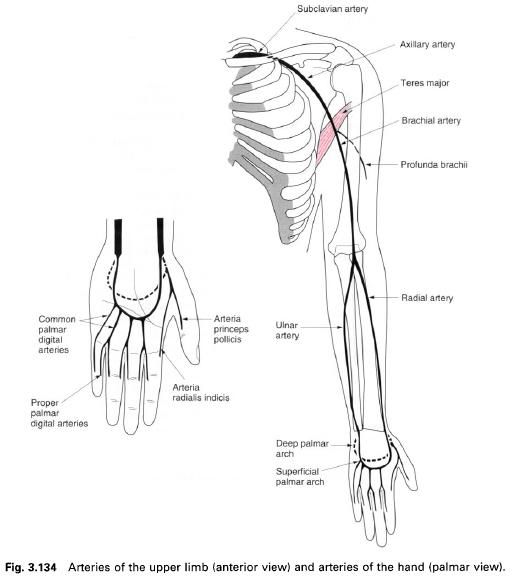
The main arterial stem of the upper limb passes
through the root of the neck, the axilla and the arm before dividing into two
in the forearm. It changes its name in each of the regions as it crosses
particular bony or muscular landmarks.
The
subclavian artery
The right subclavian artery lies entirely
within the root of the neck, having arisen from the brachiocephalic trunk. The
left subclavian artery arises from the aortic arch in the superior mediastinum
to enter the root of the neck. Both arteries pass laterally over the first rib
towards the axilla, and end by becoming the axillary artery its lateral border.
The subclavian artery is conveniently divided into three parts by scalenus
anterior which crosses it anteriorly.
In the neck, the artery runs from the upper
border of the sternoclavicular joint to the middle of the clavicle. The course is convex upwards. The artery can be
compressed against the first rib by a downward and backward pressure applied
behind the clavicle, lateral to the
posterior border of sternocleidomastoid.
Branches from the subclavian artery supply
structures within the neck, and the anterior chest wall, and give an important
supply to the brain via the vertebral artery.
The
axillary artery
The axillary artery is the continuation of the
subclavian artery at the lateral border of the first rib and ends by becoming
the brachial artery at the lower border of teres major, at the level of the lateral extremity of the posterior axillary
fold. For descriptive purposes, it is divided into three parts by pectoralis minor. However, the length of
each part will depend on the position of the arm. The cords of the brachial plexus are named according to
their position with respect to the second part of the axillary artery.
The course of the artery is represented by a
line drawn from the midpoint of the clavicle
and passing immediately below the coracoid process to the medial lip of the
intertubercular groove behind coracobrachialis.
It thus describes a curve with the concavity facing downwards and medially.
The pulse of the axillary artery is readily
palpated in the lateral wall of the axilla in the groove behind the coracobrachialis muscle. This is a
useful pressure point to control distal bleeding, although paraesthesia may
result from the inevitable pressure on the median, ulnar and radial nerves
which are in close relation to the artery at this point.
Branches from the axillary artery supply the
shoulder and pectoral regions, as well as the lateral chest wall. They
anastomose with branches from the subclavian artery and the posterior
intercostal arteries from the descending thoracic aorta. These anastomoses and
their vessels may be enlarged in conditions where there is a narrowing of the
aorta beyond the origin of the left subclavian artery(coarctation of the
aorta), and serve as a collateral system bypassing the restriction.
The
brachial artery
This is the continuation of the axillary artery
beyond the lower border of teres major
and ends in the cubital fossa opposite the neck of the radius. It lies successively on the long and medial heads of triceps, the coracobrachialis insertion and brachialis.
Anteriorly it is covered by the medial border of the biceps, and is crossed from lateral to medial by the median nerve
about halfway down the arm. In the cubital fossa it lies beneath the bicipital
aponeurosis, which separates it from the median cubital vein, with the median
nerve lying medial to the artery and with the biceps tendon lying lateral. The brachial artery divides into the
radial and ulnar arteries.
High division of the brachial artery sometimes
occurs proximal to the cubital fossa. Indeed, it may divide at any point
between the axilla and the cubital fossa, in which case the two arteries
descend side-by-side following the normal course of the brachial artery.
The brachial
pulse may be felt along the whole course of the artery by compressing it
against the humerus, directing
lateral pressure proximally and dorsolateral pressure distally. It is best felt
just medial to the bicipital aponeurosis at the level of the medial epicondyle
of the humerus, and it is at this
point that one listens for Korotkoff’s
sounds when measuring blood pressure.
A major branch of the brachial artery is the profunda brachii, which runs with the
radial nerve in the spiral groove between the lateral and medial heads of the triceps to pass into the posterior
compartment of the arm. Branches from both the brachial artery and the profunda
brachii supply the muscles of the arm and contribute to the anastomosis around
the elbow joint.
The
radial artery
The radial artery begins in the cubital fossa
opposite the neck of the radius and
ends by completing the deep palmar arch in the hand. It is usually thought of and described as having three parts.
The first part is in the forearm, the second curves laterally around the wrist
as far as the first interosseus space, and the third passes through the
interosseus space into the palm.
If the arm is placed in a midpronated position
and brachioradialis is tensed, then
the course of the first part of the radial artery may be indicated by a
slightly convex line beginning at the biceps
tendon and running down the medial side of brachioradialis
to a point just medial to the radial styloid process on the anterior aspect. As
it curves around the wrist, the radial artery is within the “anatomical
snuffbox” and lies on the radiocarpal ligament, the scaphoid and trapezium. It
is crossed by the tendons of abductorpollicis longus and extensors pollicis brevis and longus from lateral to
medial.
The third part of the artery passes between the
two heads of the first dorsal interosseus and adductor pollicis before completing the deep palmar arch.
The radial
pulses may be felt against the distal border of the radius lateral to flexor carpi radialis, and in the “anatomical snuffbox” against the scaphoid.
Branches from the first part of the artery are
involved in the elbow anastomosis and supply the muscles on the radial side of
the forearm. From the second part arise branches supplying the wrist and dorsum
of the hand and thumb. Before
completing the deep palmar arch, the third part of the artery gives off the princes pollicis and radialis indicis
branches to the thumb and index fingers respectively.
The ulnar
artery
The ulnar artery begins in the cubital fossa as
a terminal branch of the brachial artery, and ends at the pisiform by dividing
into deep and superficial palmar arteries. It may be represented by a line
passing, medially convex, from the tendon of biceps to the pisiform bone and from there to the hook of the
hamate. In its course, it lies on brachialis,
flexor digitorum profundus and the flexor retinaculum, and is crossed
anteriorly, from above downwards by: pronator teres, the median nerve, flexor carpi radialis, palmaris longus and flexor digitorum superficialis, being
overlapped lower down by flexor carpi ulnaris. Just below the radial tuberosity, the common interosseus artery is
given off, and this divides into anterior and posterior interosseus arteries
which run down either side of the interosseus membrane, supplying the deep
muscles of both flexor and extensor compartments. Branches from the proximal
and distal ends of the artery are involved in the supply to the elbow and wrist
joints respectively.
The
superficial palmar arch
This is formed mainly by the ulnar artery, with
a contribution from the superficial palmar branch of the radial artery. It lies
deep to the palmar aponeurosis. The distal convexity of the arch lies level
with the flexor surface of the extended thumb.
Four common
palmar digital arteries arise from the superficial arch with the most
medial running along the medial side of the little finger. The other three each
divide into two proper digital arteries which supply adjacent sides of the
little, ring, middle and index fingers.
The
deep palmar arch
This is formed mainly by the radial artery with
a contribution from the deep branch of the ulnar artery. It lies deep to the
long flexor tendons and their synovial sheaths on the bases of the metacarpals
and gives rise to the palmar metacarpal arteries. Its distal convexity is 2cm
distal to the distal crease of the wrist.







0 коментара:
Постави коментар