



If we recall that cardiac output is the product
of heart rate and stroke volume(Q = HR x
SV), cardiac output predictably
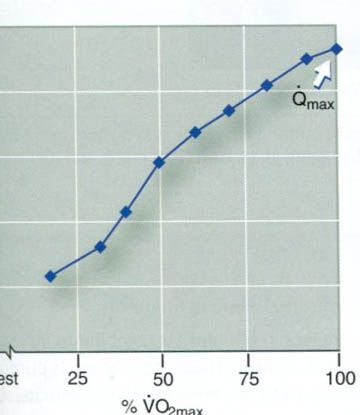
increases with increasing exercise intensity(figure below). Resting cardiac
output is approximately 5.0 L/min, but varies in proportion to the size of the
person. Maximal cardiac output varies between 20(sedentary person) and
40(elite endurance athlete) L/min and is a function of both body size and
endurance training. The linear relationship between cardiac output and intensity
of exercise is predictable because the major purpose of the increase in cardiac
output is to meet the muscles’ increased demand for oxygen. Like VO2max,
when cardiac output approaches maximal exercise intensities it may reach a
plateau. In fact, it is likely that VO2max is limited by this
leveling off of cardiac output.
The
integrated cardiac response to exercise
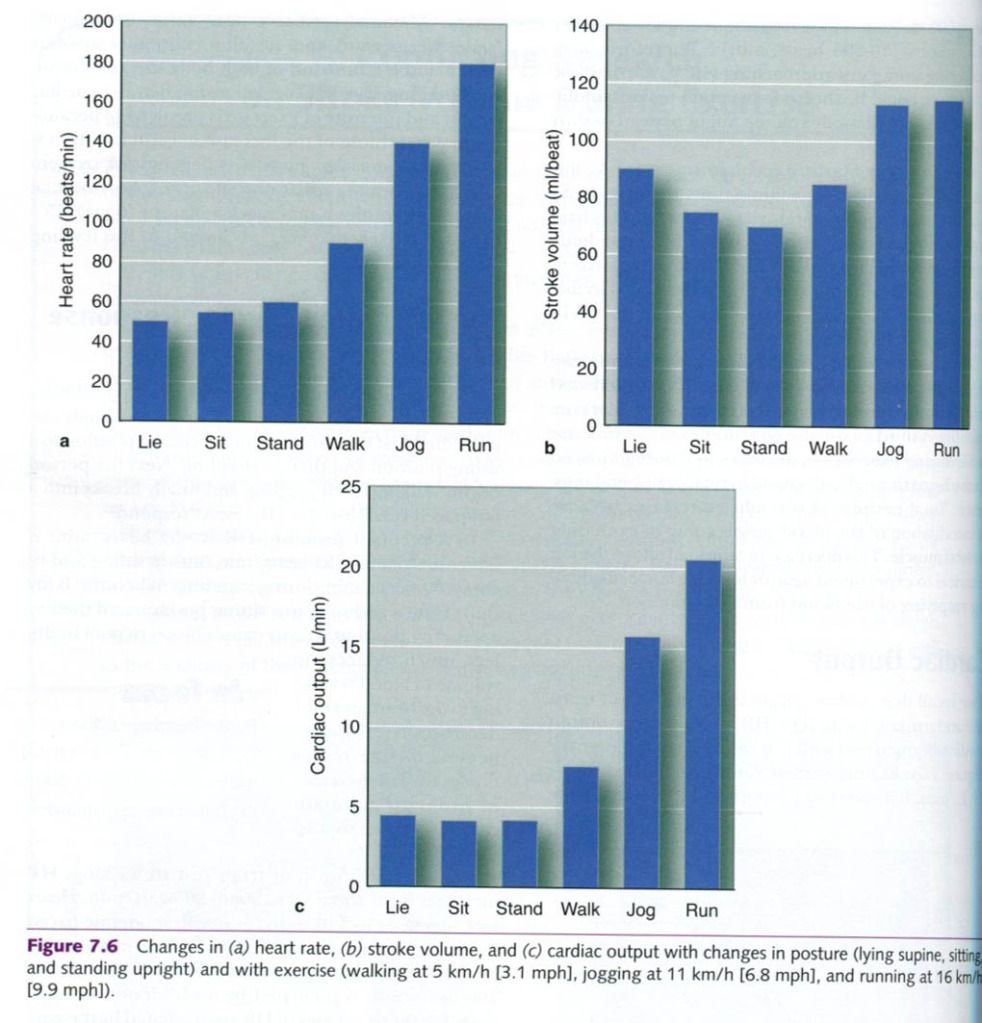
To see how HR, SV, and Q vary under various
conditions of rest and exercise, consider the following example. An individual
first transitions from a reclining position to a sitting position and then to
standing. Next the person begins walking, then jogging, and finally breaks into
a fast-paced run. How does the heart respond?
In a reclined position, HR is ~50 beats/min; it
increases to about 55 beats/min during sitting and to about 60 beats/min during
standing. When the body shifts from a reclining to a sitting position and
then to a standing position, gravity causes blood to pool in the legs, which
reduces the volume of blood returning to the heart and thus decreases SV. To
compensate for the reduction in SV, HR increases in order to maintain cardiac
output; that is, Q = HR x SV.
During the transition from rest to walking, HR
increases from about 60 to about 90 beats/min. Heart rate increases to 140
beats/min with moderate-paced jogging and can reach 180 beats/min or more with
a fast-paced run. The initial increase in HR up to about 100 beats/min is
mediated by a withdrawal of vagal tone. Further increases in HR are mediated by th sympathetic nervous system.
Stroke volume also increases with exercise, further increasing cardiac output.
These relationships are shown in the picture below.
During the initial stages of exercise in
untrained individuals, increased cardiac output is caused by an increase in
both HR and SV. When the level of exercise exceeds 40% to 60% of the
individual’s maximal exercise capacity. SV either plateaus or continues to
increase, but at a much slower rate. Thus, further increases in cardiac output
are largely the result of increases in HR. Stroke volume increases are likely
to contribute more to the rise in cardiac output during the higher intensities
of exercise in those people who are highly trained.
Blood pressure
During dynamic exercise, mean arterial blood pressure
increases substantially. However, systolic and diastolic blood pressure do not
increase to a similar degree. With whole-body endurance exercise, systolic
blood pressure increases in direct proportion to the increase in exercise
intensity. However, diastolic pressure does not change significantly, and may
even decrease. A systolic pressure that starts out at 120mmHg in a normal
healthy person at rest can exceed 200mmHg at maximal exercise. Systolic
pressures of 240 to 250mmHg have been reported in normal, healthy, highly
trained athletes at maximal intensities of aerobic exercise.
Increased systolic blood pressure results from
the increased cardiac output(Q) that accompanies increasing rates of work. This
increase in pressure helps facilitate the increase in blood flow through the
vasculature. Also, blood pressure(that is, hydrostatic pressure) determines how
much plasma leaves the capillaries, entering the tissues and carrying needed
supplies. Thus increased systolic pressure aids substrate delivery to working
muscles.
Blood pressure reaches a steady state during
submaximal steady-state endurance exercise. As work intensity increases, so
does systolic blood pressure. If steady-state exercise is prolonged, the
systolic pressure might start to decrease gradually, but diastolic pressure
remains constant. The slight decrease in systolic blood pressure, if it occurs,
is a normal response and simply reflects increased arteriole dilation in the
active muscles, which decreases the
total peripheral resistance or TPR(since blood pressure = cardiac output x
total peripheral resistance).
Diastolic blood pressure changes little during
submaximal dynamic exercise; however, at maximal exercise intensities,
diastolic blood pressure increases slightly. Remember that diastolic pressure
reflects the pressure in the arteries when the heart is at rest(diastole). With
dynamic exercise there is an overall increase in sympathetic neural tone to the
vasculature, causing overall vasoconstriction. However, this vasoconstriction is
blunted in the exercising muscles by the release of local vasodilators. Thus,
there is a balance between vasoconstriction to inactive regions and
vasodilatation in the active skeletal muscle; therefore diastolic pressure does
not change substantially. However, in some cases of cardiovascular disease,
increases in diastolic pressure of 15mmHg or more occur in response to exercise
and are one of several indications for immediately stopping a diagnostic
exercise test. Figure below illustrates a typical blood pressure response to
leg and arm cycling exercise with increasing exercise intensities.
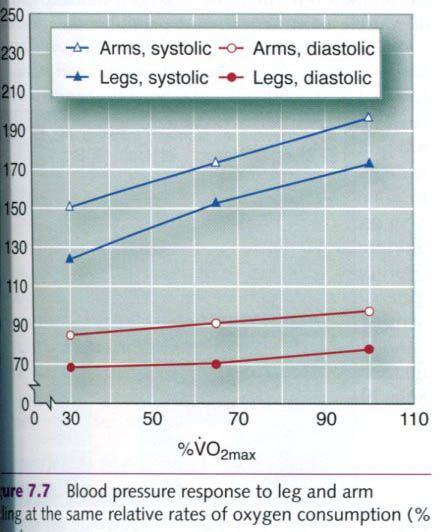
As seen in figure, upper body exercise causes a
greater blood pressure response than leg exercise at the same absolute rate of
energy expenditure. This is most likely attributable to the smaller muscle mass
and vasculature of the upper body compared with the lower body, plus an
increased energy demand to stabilize the body during arm exercise. This
difference in the systolic blood pressure response to upper and lower body
exercise has important implications for the heart. Myocardial oxygen uptake and
myocardial blood flow are directly related to the product of HR and systolic
blood pressure. This value is referred to as the rate-pressure product or
double product(DP = HR x SBP). With static or dynamic resistance exercise or
upper body work, the rate-pressure product is elevated , indicating increased
myocardial oxygen demand. This relationship between rate-pressure product and
myocardial oxygen demand is important in clinical exercise testing.
Blood pressure responses to resistance
exercise, such as weighlifting, are exaggerated. With high-intensity resistance
training, blood pressure can reach 480/350mmHg. In such exercise, use of the
Valsalva maneuver is quite common. This maneuver occurs when a person tries to
exhale while the mouth, nose, and glottis are closed. This action causes an
enormous increase in intrathoracic pressure. Much of subsequent blood pressure
increase results from the body’s effort to overcome the high internal pressures
created during the Valsalva maneuver.












0 коментара:
Постави коментар