



- Heart rate
- Stroke volume
- Cardiac output
- Blood pressure
- Blood flow
- Blood.
Heart
rate(HR) is one of the
simplest and yet most informative of the cardiovascular parameters. Measuring HR involves simply taking the
subject’s pulse, usually at the radial or carotid artery. Heart rate is a
good indicator of the intensity of
exercise.
Resting
heart rate
Resting heart rate(RHR) averages 60 to 80 beats/min in most individuals. In highly
conditioned, endurance-trained athletes, resting rates as low as 28 to 40
beats/min have been reported. This is mainly due to an increase in vagal tone
that accompanies endurance exercise training. Resting heart rate can also be
affected by environmental factors, for example, it increases with extremes in
temperature and altitude.
Just before the start of exercise, preexercise
HR usually increases above normal resting values. This is called an anticipatory response. This response is
mediated through release of the neurotransmitter norepinephrine from the
sympathetic nervous system and the hormone epinephrine from the adrenal
medulla. Vagal tone probably also decreases. Because preexercise HR is
elevated, reliable estimates of the true RHR should be made only under
conditions of total relaxation, such as early in the morning before the subject
rises from a restful night’s sleep.
Heart
rate during exercise
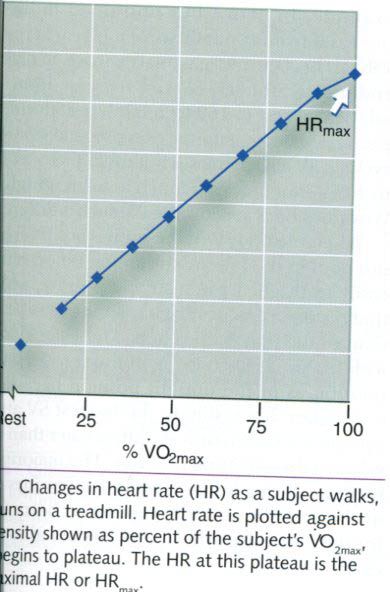
When exercise begins, HR increases directly in
proportion to the increase in exercise intensity(see picture below), until
near-maximal exercise is achieved. As maximal exercise intensity is approached,
HR begins to plateau even as the
exercise workload continues to increase. This indicates that HR is approaching
a maximum value. The maximum heart
rate(HRmax) is the highest HR value achieved in an all-out effort to the point of exhaustion.
This is a highly reliable value that remains constant from day to day. However,
this value changes slightly from year to year due to the normal age-related
decline in HRmax.
HRmax is often estimated based on
age because HRmax shows a slight but steady decrease of about one
beat per year beginning at 10 to 15 years of age. Subtracting one’s age from 220 provides an approximation of one’s
average HRmax. However, this is only an estimate – individual values
vary considerably from this average value. To illustrate, for a
40-year-old person, HRmax would be estimated to be 180 beats/min(HRmax
= 220-40). However, 68% of all 40-year-olds have actual HRmax values
between 168 and 192 beats/min(mean ±1 standard deviation), and 95% fall between
156 and 204 beats/min(mean ±2 standard deviations). This demonstrates the
potential for error in estimating a person’s HRmax. A more accurate
equation has been developed to estimate HRmax from age. In this
equation, HRmax = 208 –
(0.7 x age).
When the rate of work is held constant at a
submaximal intensity, HR increases fairly rapidly until it reaches a plateau. This
plateau is the steady-state heart
rate, and it is optimal HR for meeting the circulatory demands at that specific
rate of work. For each subsequent increase in intensity, HR will reach a new
steady-state value within 2 to 3 min. However, the more intense the exercise,
the longer it takes to achieve this steady-state value.
The concept of steady-state heart rate forms
the basis for several tests that have been developed to estimate physical
fitness. In one such test, individuals are placed on an exercise device, such
as a cycle ergometer, and then perform exercise at two or three standardized
exercise intensities. Those in better physical condition(i.e., those with
better cardiorespiratory endurance capacity) will have a lower steady-state HR
at each exercise intensity than those who are less fit. Thus, steady-state
HR is a valid predictor of cardiorespiratory fitness: A lower steady-state HR
reflects greater cardiorespiratory fitness.
Figure below illustrates results from a
submaximal exercise test performed by two different individuals of the same
age. Steady-state HR is measured at three to four distinct workloads, and a
line of best fit is drawn through the data points. Because there is a
consistent relationship between intensity and energy demand, steady-state HR
can be plotted versus the corresponding energy(VO2) required to do
work on the cycle ergometer. The resultant line can be extrapolated to the
age-predicted HRmax to estimate an individual’s maximal exercise
capacity. In this picture, subject A has a higher fitness level than subject B
because at any given submaximal intensity, his HR is lower; and extrapolation
to age-predicted HRmax yields a higher estimated maximal exercise
capacity(VO2max).

Stroke volume(SV) also changes during acute
exercise to allow the heart to meet the demands of exercise. At near-maximal
and maximal exercise intensities, SV is a major determinant of
cardiorespiratory endurance capacity.
Stroke volume is determined by four factors:
1) The
volume of venous blood returned to the heart(the heart can only pump what
returns: preload)
2) Ventricular
distensibility(the capacity to enlarge the ventricle, for
maximal filling)
3) Ventricular
contractility(the inherent capacity of the ventricle to
contract)
4) Aortic
or pulmonary artery pressure(the pressure against which the ventricles must
contract: afterload).
The first two factors influence the filling
capacity of the ventricle, determining how much blood is available for filling
the ventricle and the ease with which the ventricle is filled at the available
pressure. This is reffered to preload.
The last two factors influence the ventricle’s ability to empty, determining
the force with which blood is ejected and the pressure, or afterload, against which it must be expelled into the arteries.
These four factors directly control the alterations in SV in response to
increasing exercise intensity.
Stroke
volume increase with exercise
Stroke volume increases above resting values
during exercise. Most researchers agree that SV increases with increasing rates
of work, but only up to exercise intensities somewhere between 40% and 60% of maximal capacity. At that point, SV
typically plateaus, remaining essentially unchanged up to and including the
point of exhaustion in the picture below. However, other researchers have
reported that SV continues to increase up through maximal exercise intensities.

When
the body is in an upright position, SV can almost double from resting to
maximal values. For
example, in active but untrained individuals, SV increases from about 60 to 70
ml/beat at rest to 110 to 130ml/beat during maximal exercise. In highly trained
endurance athletes, SV can increase from 80 to 110ml/beat at rest to 160 to
200ml/beat during maximal exercise. During supine exercise, such as recumbent
cycling, SV also increases but usually by only about 20% to 40% - not nearly as
much as in an upright position. Why does body position make such a difference?
When the body is in the supine position, blood does not pool in the lower extremities. Blood returns more easily to the heart in a supine posture, which means that resting SV values are higher in the supine position than in the upright position. Thus, the increase in SV maximal exercise is not as great in the supine position than in the upright position. Thus, the increase in SV with maximal exercise is not as great in the supine position as in the upright position because SV starts out higher. Interestingly, the highest SV attainable in upright exercise is only slightly greater than the resting value in the reclining position. The majority of the SV increase during low to moderate intensities of exercise in the upright position appears to be compensating for the force of gravity that causes blood to pool in the extremities.
When the body is in the supine position, blood does not pool in the lower extremities. Blood returns more easily to the heart in a supine posture, which means that resting SV values are higher in the supine position than in the upright position. Thus, the increase in SV maximal exercise is not as great in the supine position than in the upright position. Thus, the increase in SV with maximal exercise is not as great in the supine position as in the upright position because SV starts out higher. Interestingly, the highest SV attainable in upright exercise is only slightly greater than the resting value in the reclining position. The majority of the SV increase during low to moderate intensities of exercise in the upright position appears to be compensating for the force of gravity that causes blood to pool in the extremities.
Explanations
for the stroke volume increase
One explanation for the increase in SV with
exercise is that the primary factor determining SV is increased preload or the
extent to which the ventricle fills with blood and stretches. When the
ventricle stretches more during filling, it subsequently contracts more
forcefully. For example, when a
larger volume of blood enters and fills the ventricle during diastole, the
ventricular walls stretch. To eject that greater volume of blood, the ventricle
responds by contracting more forcefully. This is reffered to Frank-Starling mechanism. Additionally,
SV can increase during exercise if the ventricle’s contractility is enhanced by
an increase in neural stimulation, an increased release of circulating catecholamines(epinephrine,
norepinephrine), or both, even without an increased end-diastolic volume. These
mechanisms combine to increase SV during dynamic exercise.
Some clinically used cardiovascular diagnostic
techniques have made it possible to determine exactly how SV changes with
exercise. Echocardiography(using sound waves) and radionuclide
techniques(“tagging” of red blood cells with radioactive tracers) have
elucidated how the heart chambers respond to increasing oxygen demands during
exercise. With either technique, continuous pictures can be taken of the heart
at rest and up to near-maximal intensities of exercise.
Figure below illustrates the results of one
study of normally active but untrained subjects. In this study, participants
were tested during both supine and upright cycle ergometry under four
conditions, which are depicted on the x-axis:
- Rest
- Low-intensity exercise
- Intermediate-intensity
exercise
- Peak-intensity exercise.
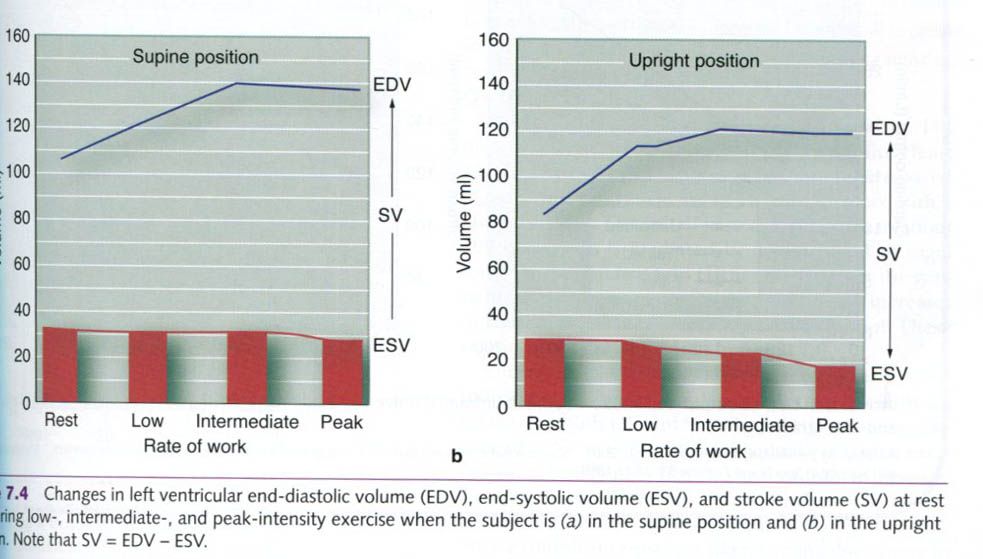
Going from resting conditions to exercise of
increasing intensities, there is an increase in left ventricular end-diastolic
volume(a greater filling or preload), indicating that the Frank-Starling
mechanism is operating. There is also a decrease in the left ventricular
end-systolic volume(greater emptying), indicating an increased degree of
contractility.
This figure shows that both the Frank-Starling
mechanism and increased contractility are important in increasing SV during
exercise. The Frank-Starling mechanism appears to have its greatest influence
at lower exercise intensities, and contractility has its greates effects at
higher exercise intensities.
Recall that HR also increases with exercise
intensity. The plateau or small decrease in left ventricular end-diastolic
volume at higher exercise intensities could be caused by reduced ventricular
filling time. One study showed that ventricular filling time decreased from
about 500 to 700ms at rest to about 150ms at higher HRs(about 150-200
beats/min). Therefore, with increasing work rates approaching HRmax,
the diastolic filling time could be shortened enough to limit filling. As a
result, end-diastolic volume might plateau or start to decrease.
For the Frank-Starling mechanism to work, left
ventricular end-diastolic volume must increase by an increase in venous blood
return to the heart. This happens through redistribution of blood by
sympathetic through redistribution of blood by sympathetic activation of
arteries and arterioles in inactive areas of the body such as in the renal and
splanchnic circulations. Also, the muscle and respiratory pumps aid in
increasing venous return.
Thus, two factors that can contribute to an
increase in SV with increasing intensity of exercise are increased venous
return(preload) and increased ventricular contractility. A third factor also
contributes to the increase in SV during exercise - a decrease in afterload placed on the heart
through a decrease in total peripheral resistance. Total peripheral resistance
decreases because of vasodilatation of the blood vessels going to exercising
skeletal muscle. This decrease in afterload allows the left ventricle to expel
blood against less resistance, facilitating emptying of the blood from this
chamber.












0 коментара:
Постави коментар