



Blood flow through the heart
The
heart is sometimes considered to be two separate pumps, with the right side of
the heart pumping deoxygenated blood to the lungs through the pulmonary
circulation and the left side of the heart pumping oxygenated blood to all
other tissues in the body through the systemic circulation. Blood that has
circulated through the body, delivering oxygen and nutrients and picking up
waste products, returns to the heart through the great veins – the superior
vena cava and inferior vena cava – to the right atrium. This chamber receives
all the deoxygenated blood from the systemic circulation.
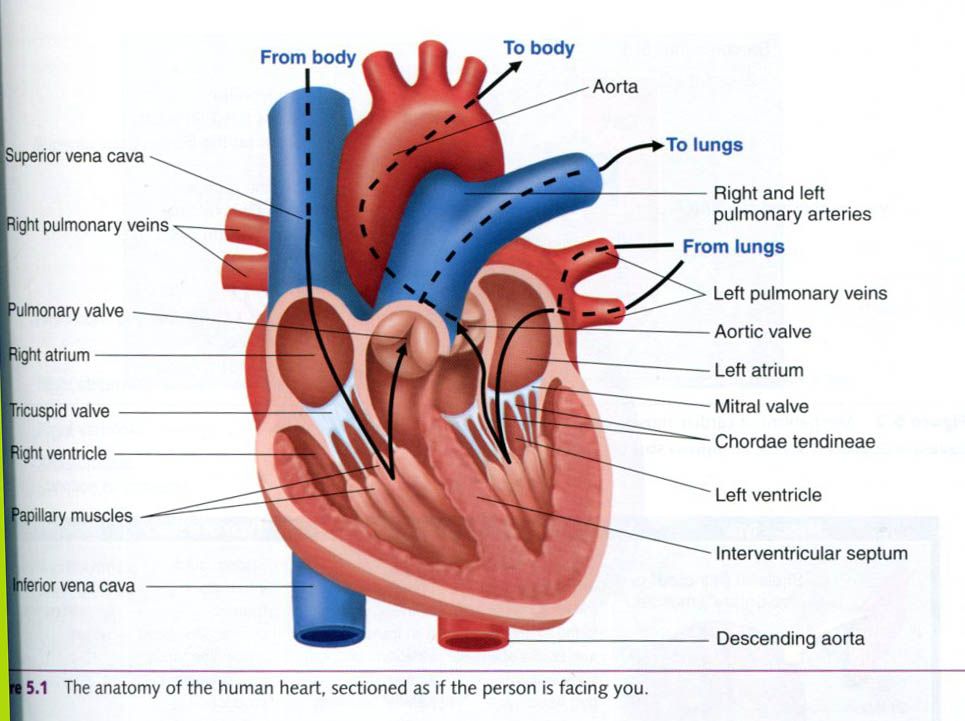
From
the right atrium, blood passes through the tricuspid valve into the right
ventricle. This chamber pumps the blood through
the pulmonary valve into the pulmonary artery, which carries the blood
to the lungs. Thus, the right side of the heart is known as the pulmonary side,
sending the blood that has circulated throughout the body into the lungs for
reoxygenation.
After
blood is oxygenated in the lungs, it is transported back to the heart through
the pulmonary veins. All freshly oxygenated blood is received from the
pulmonary veins by the left atrium. From the left atrium, the blood passes
through the mitral valve into the left ventricle. Blood leaves the left
ventricle by passing through the aortic valve into the aorta and is distributed
to the systemic circulation. The left side of the heart’s known as the systemic
side. It receives the oxygenated blood from the lungs and then sends it out to
supply all other body tissues.
Myocardium
Cardiac muscle is collectively called the
myocardium, or myocardial muscle. Myocardial thickness at various locations in
the heart varies according to the amount of stress placed on it. The left
ventricle is the most powerful of the four heart chambers. This chamber must
contract to generate sufficient pressure to pump blood through the entire body.
When a person is sitting or standing, the left ventricle must contract with
enough force to overcome the effect of gravity, which tends to pool blood in
the lower extremities.
The left ventricle must generate a considerable
amount of force to pump blood to the systemic circulation, and this is
reflected by the greater thickness of its muscular wall compared with that of
the other heart chambers. This hypertrophy is the result of the pressure placed
on the left ventricle at rest or under normal conditions of moderate activity.
With more vigorous exercise – particularly intense aerobic activity, during
which the working muscles’ need for blood increases considerably – the demand
on the left ventricle to deliver blood to exercising muscle is high. In response to both intense aerobic and
resistance training, the left ventricle will hypertrophy. In contrast to
the positive adaptations that occur as a result of physical training, cardiac
muscle also hypertrophies as a result of diseases, such as high blood pressure
or valvular heart disease. In response to either training or disease, over time the left ventricle adapts by
increasing its size and pumping capacity, similar to the way skeletal muscle
adapts to physical training. However, the mechanisms for adaptation and
cardiac performance with disease are different from those observed with aerobic
training.
Although striated in appearance, the myocardium
differs from skeletal muscle in several important ways. First, cardiac
muscle fibers are anatomically interconnected end to end by dark-staining
regions called intercalated disks.
These disks have desmosomes, which are structures that anchor the individual
cells together so that they do not pull apart during contraction, and gap
junctions, which allow rapid transmission of the action potentials that signal
the heart to contract as one unit. Secondly, the myocardial fibers are rather
homogenous in contrast to the mosaic of fiber types in skeletal muscle. The
myocardium contains only one fiber type, thought to be similar to type I fibers
in skeletal muscle in that it is highly oxidative, is highly capillarized, and
has a large number of mitochondria.
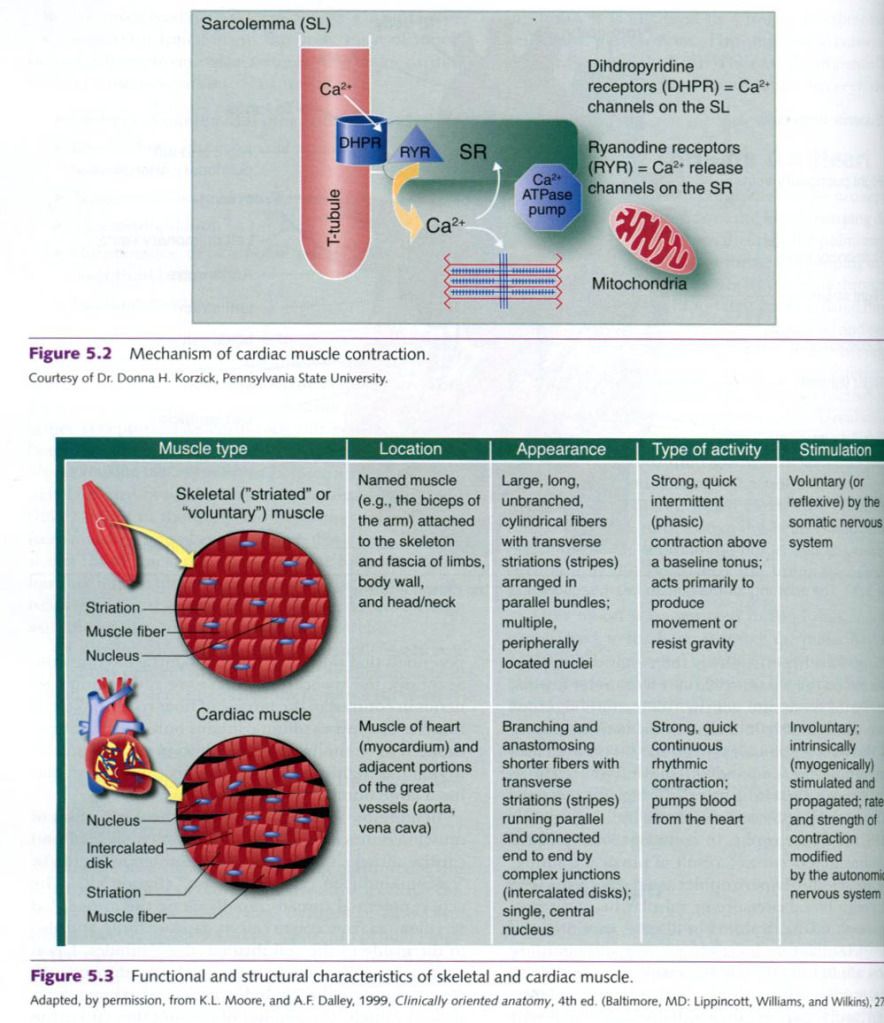
In addition to these differences, the mechanism
of muscle contraction also differs between skeletal and cardiac muscle. Cardiac
muscle contraction occurs by “calcium-induced calcium release”. The action
potential spreads rapidly along the myocardial sarcolemma from cell to cell via
gap junctions, and also to the inside of cell through the T-tubules. Upon
stimulation, calcium enters the cell
by the dihydropyridine receptor in the T-tubules. Unlike what happens in skeletal
muscle, the amount of calcium that enters the cell is not sufficient to
directly cause the cardiac muscle to contract; but it serves as a trigger to
another type of receptor, called the ryanodine receptor, to release calcium
from the sarcoplasmic reticulum. Figure below also summarizes and differences
between cardiac and skeletal muscle.
The
myocardium, just like skeletal muscle, must have a blood supply to deliver
oxygen and nutrients and remove waste products. Although blood courses through
each chamber or the heart, little nourishment comes from this blood supply. The
primary blood supply to the heart is provided by the right and left coronary
arteries, which arise from the base of the aorta and encircle the outside of
the myocardium.
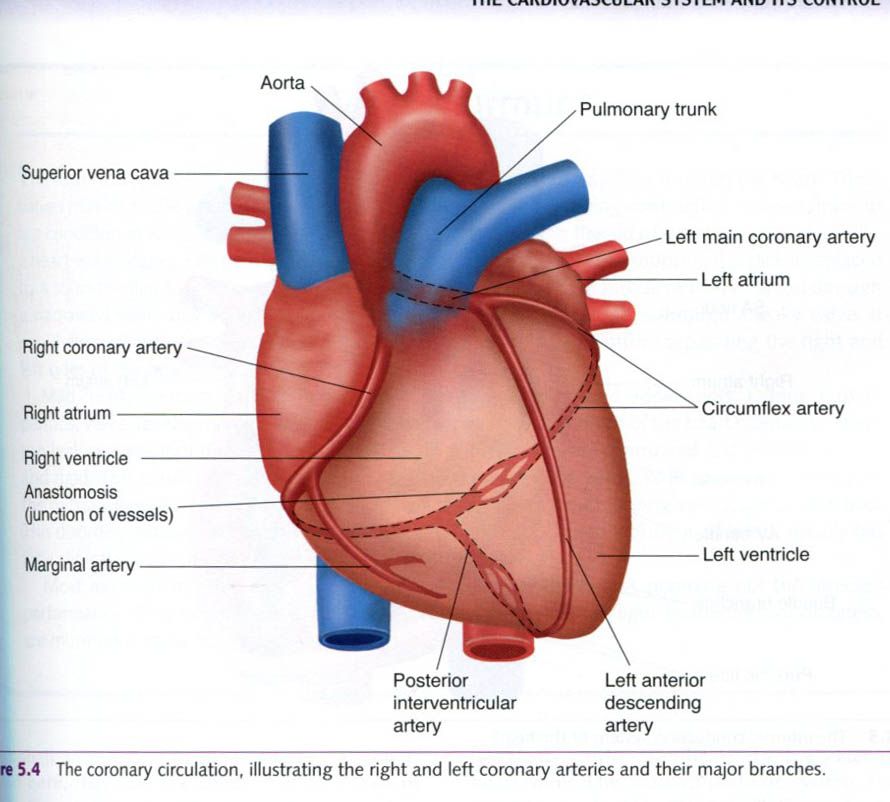
The right coronary artery supplies the right side of the heart,
dividing into two primary branches, the marginal artery and the posterior
interventricular artery. The left coronary artery, also referred to as the left
main coronary artery, also divides into two major branches, the circumflex
artery and the anterior descending artery. The posterior interventricular
artery and the anterior descending artery merge, or anastomose, in the lower
posterior area of the heart, as does the circumflex. These arteries are very susceptible to
atherosclerosis, or narrowing by the accumulation of plaque and inflammation,
leading to coronary artery disease. Anomalies – shortenings, blockages, or
misdirections – sometimes occur in the coronary arteries, and such congenital
abnormalities are a common cause of sudden death in athletes.
The ability of the myocardium to contract as a
single unit depends on initiation and propagation of an electrical signal
through the heart, the cardiac contraction system.
Cardiac conduction system
Cardiac muscle has the unique ability to
generate its own electrical signal, called spontaneous rhytmicity, which allows
it to contract without any external stimulation. The contraction is rhythmical,
in part because of the anatomical coupling of the conduction cells through gap
junctions. With neither neural nor hormonal stimulation, the intrinsic heart
rate(HR) averages – 100 beats (contractions) per minute. This resting heart
rate of about 100 beats/min can be observed in patients who have undergone
cardiac transplant surgery, because their transplanted hearts lack neural
innervation.
Figure below illustrates the four main
components of the cardiac conduction system:
- Sinoatrial(SA) node
- Atrioventricular(AV) node
- AV bundle(bundle of His)
- Purkinje fibers.
The
impulse for normal heart contractions is initiated in the sinoatrial(SA) node,
a group of specialized cardiac muscle fibers located in the upper posterior
wall of the right atrium. These specialized cells spontaneously depolarize at a
faster rate than other myocardial muscle cells because they are especially
leaky to sodium. Because this tissue generates the electrical impulse,
typically at a frequency of about 100 beats/min – the fastest intrinsic firing
rate – the SA node is known as the heart’s pacemaker, and the rhythm it
establishes is called the sinus rhythm. The electrical impulse generated by the
SA node spreads through both atria and reaches the atrioventricular(AV) node,
located iin the right atrial wall near the center of the heart. As the electrical
impulse spreads through the atria, they are signaled to contract.

The
AV node conducts the electrical impulse from the atria into the ventricles. The
impulse is delayed by about 0.13s as it passes through the AV node, and then it
enters the AV bundle. This delay allows blood from the atria to completely
empty into the ventricles to maximize ventricular filling before the ventricles
contract. While most blood moves passively from the atria to the ventricles,
active contraction of the atria(sometimes called the “atrial kick”) completes
the process. The AV bundle travels along the ventricular septum and then sends
right and left bundle branches into both ventricles. These branches send the
impulse toward the apex of the heart and then outward. Each bundle branch
subdivides into many smaller ones that spread throughout the entire ventricular
wall. These terminal branches of the AV bundle are the Purkinje fibers. They
transmit the impulse through the ventricles approximately six times faster than
through the rest of the cardiac conduction system. This rapid conduction allows
all parts of the ventricle to contract at virtually the same time.
Occasionally,
chronic problems develop within the cardiac conduction system, hampering its
ability to maintain appropriate sinus rhythm throughout the heart. In such
cases, an artificial pacemaker can be surgically installed. This small,
battery-operated electrical stimulator, usually implanted under the skin, has
tiny electrodes attached to the right ventricle. An electrical stimulator is
useful, for example, to treat a condition called AV block. With this disorder,
the SA node creates an impulse, but the impulse is blocked at the AV node and
cannot reach the ventricles, resulting in the heart rate’s being controlled by
the intrinsic firing rate of the pacemaker cells in the ventricles(closer to 40
beats/min). The artificial pacemaker takes over the role of the disabled AV
node, supplying the needed impulse and thus controlling ventricular
contraction.
Extrinsic control of heart activity
Although the heart initiates its own electrical
impulses(intrinsic control), both the rate and effect can be altered. Under
normal conditions, this is accomplished primarily through three extrinsic
systems:
- The parasympathetic nervous
system
- The sympathetic nervous
system
- The endocrine system(hormones)
The
parasympathetic system, a branch of the autonomic nervous system, originates
centrally in a region of the brain stem called the medulla oblongata and
reaches the heart through the vagus nerve(cranial nerve X). The vagus nerve
carries impulses to the SA and AV nodes, and when stimulated releases
acetylcholine, which causes hyperpolarization of the conduction cells. The
result is a decrease in a heart rate. At rest, parasympathetic system activity
predominates and the heart is said to have “vagal tone”. Recall that, in the
absence of vagal tone, intrinsic heart rate would be approximately 100
beats/min. The vagus nerve has a depressant effect on the heart: it slows
impulse generation and conduction and thus decreases the heart rate. Maximal
vagal stimulation can decrease the heart rate to as low as 20 to 30 beats/min.
The vagus nerve also decreases the force of cardiac muscle contraction.
The
sympathetic nervous system, the other branch of the autonomic system, has
opposite effects. Sympathetic stimulation increases the rate of impulse
generation and conduction speed, and thus heart rate. Maximal sympathetic
stimulation allows the heart rate to increase up to 250 beats/min. Sympathetic
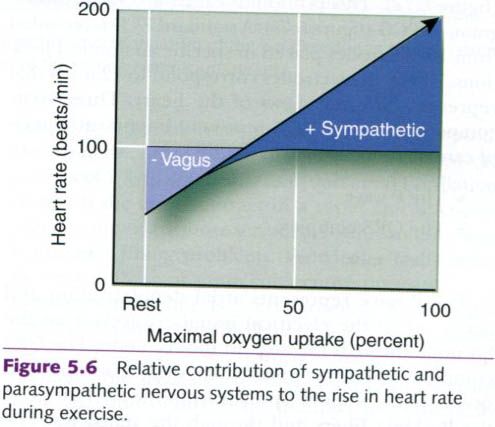
input also increases the contraction force of the ventricles. The sympathetic
system predominates during times of physical or emotional stress, when the
heart rate is greater than 100 beats/min. The parasympathetic system dominates
when heart rate is less than 100. Thus, when exercise begins, or if exercise is
at a low intensity, heart rate first increases due to withdrawal of vagal tone,
with further increases if necessary due to sympathetic activation, as shown in the figure below.
The third extrinsic influence, the endocrine
system, exerts its effect through two hormones released by the adrenal medulla:
norepinephrine and epinephrine.
These hormones are also known as catecholamines. Like norepinephrine that
serves as the major neurotransmitter in the sympathetic nervous system,
norepinephrine and epinephrine stimulate the heart, increasing its rate and
contractility. In fact, release of these hormones from the adrenal medulla is
triggered by sympathetic stimulation during times of stress, and their actions
prolong the sympathetic response.
Normal resting heart rate(RHR) typically varies
between 60 and 100 beats/min. With extended periods of endurance
training(months to years), the RHR can decrease to 35 beats/min or less. A RHR
as low as 28 beats/min has been observed in a world class, long-distance
runner. These lower training-induced RHRs are postulated to result from
increased parasympathetic stimulation(vagal tone), with reduced sympathetic
activity playing a lesser role.






0 коментара:
Постави коментар