



31. 5. 2013.
29. 5. 2013.
Muscles dorsiflexing the ankle
Tibialis anterior
Extensor digitorum longus
Extensor hallucis longus
Peroneus tertius
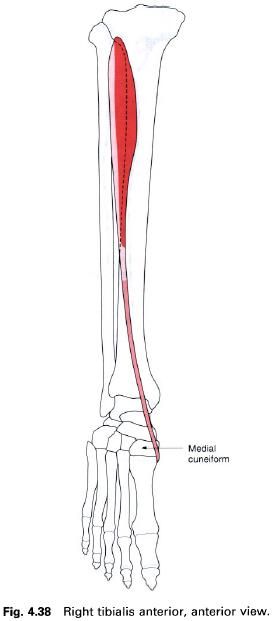
Tibialis anterior
Tibialis anterior is a long fusiform muscle
situated on the front of the leg lateral to the anterior border of the tibia. It is covered by strong fascia
and gains its upper attachment from the deep surface of this fascia, the upper two-thirds of the lateral surface of the tibia and the adjoining part of the interosseus membrane. The muscle becomes
tendinous in its lower third, passing downwards and medially over the distal
end of the tibia. The tendon
continues through both the superior and inferior extensor retinaculae to insert
into the medial side of the medial cuneiform and base of the first metatarsal, the insertion reaching the under surface of both
bones to blend with that of peroneus longus.
Nerve
supply
This muscle is supplied by the deep peroneal nerve, root value L4, 5.
The skin covering the muscle is also supplied by roots L4, 5.
Action
Tibialis anterior is a dorsiflexor of the foot at the ankle joint. When working
with tibialis posterior it acts as an
invertor of the foot, in which the
sole of the foot is turned to face
medially.
Functional
activity
As with other muscles in the leg, tibialis
anterior is concerned with balancing the body on the foot. It works with the surrounding muscles to maintain body
balance during activities of the upper part of the body which change the
distribution of weight.
Not only is tibialis anterior responsible for
dorsiflexing the foot as the lower
limb is carried forward during the swing-through phase of walking, so
preventing the toes catching the ground, it also controls the placement of the foot on the ground following initial
ground contact by the heel. On close observation, especially in slow motion, it
will be seen that the heel does not strike the ground and remain immobile at
the initiation of the stance phase, but glides on to the surface and acts as
the first braking force of the lower limb’s forward movement. Overactivity of
tibialis anterior accounts for the wear patterns seen on the posterolateral
aspect of the heel, due to the frictional forces between the shoe and the
ground. The rest of the foot is then
gradually lowered to the ground in a controlled manner taking up the
undulations of the surface concerned. The landing of the foot on the ground is similar to the landing of an aeroplane; the
main wheels touch down first applying the initial braking force followed by a
controlled lowering of the front of the craft as the speed decreases.
Tibialis anterior in association with the other
dorsiflexors, therefore, plays an important part in the lowering of the
forefoot to the ground in walking or running and will be put under stress in
extended activity particularly over rough terrain. The anterior calf muscles
are enclosed in particularly tight fascia which allows very little expansion of
the tissues. The result is a compression of the muscle during activity and a
dragging on the attachments of the surrounding fascia, particularly where it
attaches to the bone. This leads to a painful condition of this area commonly
called “shin splints”.
Paralysis of tibialis anterior causes footdrop
because the remaining dorsiflexors are not strong enough to raise the toes and
so prevent them dragging along the ground. The patient may overcome this by
flexing the knee more than normal during walking or by fitting a “toe-raise”
orthosis to patients or their shoe.
Palpation
Both the muscle belly and tendon can be seen
and felt when the foot is dorsiflexed
against resistance, the tendon being the most medial at the ankle joint.
Extensor digitorum longus
Extensor digitorum longus is again situated on
the anterior aspect of the leg, being lateral to tibialis anterior, and
overlying extensor hallucis longus. It has a linear origin from the upper-two thirds of the anterior surface of the fibula, the deep fascia and the upper
part of the interosseus membrane with its upper fibres reaching across the lateral condyle of the tibia in conjunction with those of peroneus longus. It is a pennate muscle
with the tendon appearing on the medial side; the muscle fibres pass downwards
and medially to reach it. The tendon passes over the front of the ankle joint
deep to the superior extensor retinaculum and then through the loop of inferior
extensor retinaculum accompanied by peroneus tertius. At the level of the
inferior extensor retinaculum or immediately distal, it gives rise to four
tendons which run to the lateral four toes. The four separate tendons are
enclosed in a common synovial sheath at the level of the inferior extensor
retinaculum. On the dorsal surface of the proximal phalanx, each tendon forms a
triangular membranous expansion, known as the extensor hood (dorsal digital expansion). Each hood is joined on
its medial side by the tendon of the lumbrical and on the lateral side for the
second to fourth toes by the tendon of extensor digitorum brevis. The
interossei of the foot do not have an attachment to the extensor hood.
As the hood passes forwards over the proximal
phalanx it divides into three parts before reaching the dorsum of the proximal
interphalangeal joint. The central portion attaches to the base of the middle phalanx, while the two outer
portions unite before inserting on to the base of the distal phalanx. An attachment of the extensor hood to the dorsal
aspect of the proximal phalanx has also been described.
Nerve
supply
This muscle is supplied by the deep peroneal nerve, root value L5, S1.
The skin covering the muscle is supplied by root L5.

Action
As its name implies, extensor digitorum longs
is an extensor of the lateral four toes at the metatarsophalangeal joints, and
also assists in extension at the interphalangeal joints. However it is unable
to perform the latter action unaided, which is primarily performed by the
lumbricals. If the lumbricals are paralysed, extensor digitorum longus produces
hyperextension of the metatarsophalangeal joint, while the interphalangeal
joints become flexed. As the muscle passes across the front of the ankle joint,
it also aids in dorsiflexion of the foot.
Functional
activity
During walking and running extensor digitorum
longus draws the toes upwards after they have been flexed prior to toe-off, and
keeps them clear of the ground until the heel and foot make contact with the
ground again. Unfortunately, the lateral four toes in most individuals tend to
be flexed at the proximal interphalangeal joint and extended at the distal
interphalangeal joint. Consequently extensor digitorum longus will lift the
toes in this adapted position.
Palpation
The muscle belly is easily palpated on the
anterolateral aspect of the leg. From the head of the fibula on the lateral side of the leg, just below the knee joint,
run the fingers downwards and medially for about 2cm. When raising the toes off
the floor, the muscle can be felt contracting. Now place the fingers over the
front of the ankle joint; the tendon can be identified standing out clearly,
being lateral to those of tibialis anterior and extensor hallucis longus. From
here the tendon can now either be traced upwards, under the superior part of
the extensor retinaculum to join the muscle belly, or downwards where it breaks
up into four individual tendons running towards each of the lateral four toes.
Each tendon stands clear of the metatarsophalangeal joint as it passes towards
the dorsum of the toe.
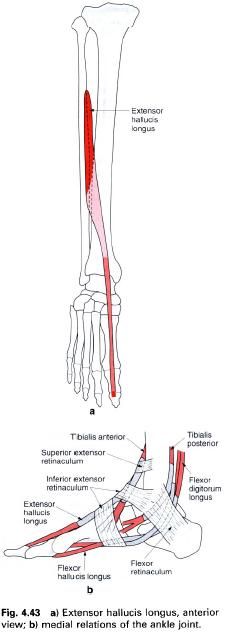
Extensor hallucis longus
Extensor hallucis longus is situated deep to
and between tibialis anterior and extensor digitorum longus on the front of the
leg. Arising from the middle half of
the anterior surface of the fibula and the adjacent interosseus membrane, the muscle fibres
pass downwards and medially to the tendon which forms on its anterior surface.
In this respect it is a unipennate muscle. The tendon passes under the superior
extensor retinaculum, through the upper part of the inferior extensor
retinaculum in a separate compartment enclosed in its own synovial sheath, and
then deep to the lower band of the inferior extensor retinaculum on its way
towards the base of the great toe. Generally, the tendon does not form a fully
developed extensor hood but passes to attach to the base of the distal phalanx
on its dorsal surface. Tendinous slips may be given off to the dorsal aspect of
the base of the proximal phalanx and the first metatarsal.
Nerve
supply
Extensor hallucis longus is supplied by the deep peroneal nerve, root value L5, S1.
The skin covering this area is supplied by roots L4, 5.
Action
As its name implies, extensor hallucis longus
will extend all of the joints of the great toe, but mainly the
metatarsophalangeal joint. It is also a powerful dorsiflexor of the foot at the ankle joint.
Functional
activity
In running, the great toe is the last part of
the foot to leave the ground and therefore the final thrust will come from the
long flexors of the toes. After this, the toe must be brought back into the
extended position at the same time as the foot
is dorsiflexed and slightly inverted, ready for the heel to be placed on the
ground for the next weightbearing phase. By extending the great toe and
dorsiflexing the foot, clearance of
the surface is also achieved. It should be noted that the great toe does not
have a lumbrical muscle or interossei associated with it. Consequently, extension
of the interphalangeal joint depends entirely on extensor hallucis longus.
Paralysis of the muscle will result in flexion of the joint and buckling of the
toe during the last phase of gait, due to the unopposed action of the flexor
muscles.
Palpation
If the great toe is extended, the tendon of the
muscle is clearly visible as it crosses the first metatarsophalangeal joint to
its insertion into the base of the distal phalanx. Trace the fingers up the
tendon; it can be felt and seen crossing the anterior aspect of the ankle joint
lateral to the tendon of tibialis anterior. From here the tendon can be felt
passing upwards and laterally before passing deep to the surrounding muscles.
Continue to move the fingers upwards for another 12cm and allow them pass a
little laterally; when the great toe is rhythmically extended and flexed, the
muscle can just be felt contracting under the fingers.
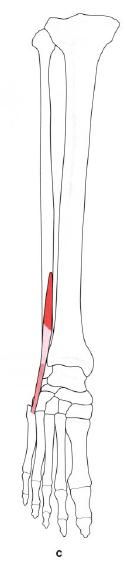
Peroneus tertius
Peroneus tertius is situated on the lower
lateral aspect of the leg and appears to have been part of extensor digitorum
longus. It arises from the front of
the lower quarter of the fibula in
continuation with the attachment of extensor digitorum longus (with no gap
between them), and from the intermuscular septum and adjoining fascia. Its
fibres pass downwards and laterally into a tendon which passes deep to the
superior and through the inferior extensor retinacula to insert into the medial
and dorsal aspect of the base of the fifth metatarsal.
Nerve
supply
Peroneus tertius is supplied by the deep peroneal nerve, root value L5, S1.
The area of skin covering the muscle is also supplied by roots L5, S1.
Action
The muscle acts as a weak evertor and
dorsiflexor of the foot at the ankle
joint.
Functional
activity
It is difficult to assess the importance of
this small muscle as its actions appear to be covered by other muscles which
have a much better mechanical leverage. Indeed in some subjects it is absent.
It does, however, pass over the anterior talofibular ligament of the ankle
joint, and it is well-known that this is very often damaged in inversion
injuries. It is therefore well placed to help prevent too much inversion during
sports activities, for example, and may be responsible for keeping down the
number of injuries. Unfortunately, the muscle is often torn and may be
completely ruptured during violent inversion, which is the cause of
considerable pain and swelling. It is possible that with the attainment of
bidepalism, peroneus tertius is assuming a more important role because eversion
of the foot is a peculiarly human
characteristic.
Palpation
Peroneus tertius is very difficult to palpate.
However, it can be felt by drawing the fingers downwards from the anterior part
of the lateral malleolus into the small hollow found there. The tendon can be
felt crossing the lateral part of the hollow to its insertion into the medial
side of the base of the fifth metatarsal. Take care not to confuse the tendon
of peroneus tertius with that of peroneus brevis, which lies lateral to this
point as it passes forwards to insert into the tubercle on the lateral side of
the fifth metatarsal.
27. 5. 2013.
Muscles plantarflexing the ankle joint
Gastrocnemius
Soleus
Plantaris
Peroneus longus
Tibialis posterior
Flexor digitorum longus
Flexor hallucis longus
Gastrocnemius
The shape of the calf is mainly due to the two
fleshy bellies of gastrocnemius( figure a), being situated on the back of the
leg with its muscle bulk mainly in the upper half. Together with soleus and
plantaris, gastrocnemius forms a composite muscle referred to as the triceps
surae. The two heads of gastrocnemius form the lower boundaries of the
popliteal fossa, which can only really be seen when the knee is flexed. The two
heads arise from the medial and lateral condyles of the femur: the medial head, from behind the medial supracondylar ridge and the adductor tubercle on the popliteal surface of the femur, the lateral head from the outer
surface of the lateral condyle of the femur
just above the behind the lateral
epicondyle. Each head has an additional attachment from the capsule of the
knee joint and from the oblique popliteal ligament, below which each head is
separated from the capsule by a bursa. The bursa associated with the medial
head often communicates with the knee joint: that under the lateral head rarely
does. There is often a sesamoid bone, the flabella, in the lateral head as it
crosses the lateral condyle of the femur.
Less commonly there may be one associated with the medial head.
From each head a fleshy bulk of muscle fibers
arise which gradually come together, although not actually blending with each
other, to insert into the posterior surface of a broad membranous tendon which
fuses with the tendon of soleus to form the upper part of the tendocalcaneus.
This broad tendon gradually narrows, becoming more rounded until it reaches
about three fingers’ breadth above the calcaneus, where it begins to expand
again and continues to do so, until its insertion into the middle part of the posterior
surface of the calcaneus. A bursa
lies between the tendon and the upper part of the calcaneus while a pad of fat
lies between the tendon and the posterior aspect of the ankle joint. Inferior
to the insertion is the fat pad of the heel.
Nerve
supply
Each head of gastrocnemius is supplied by a
branch from the tibial nerve, root
value S1, 2. The area of skin covering the muscle has roots L4, 5, S2.
Action
Gastrocnemius, together with soleus, is the
chief plantarflexor of the ankle joint. It provides the propelling force for
locomotion. As it crosses the knee joint, gastrocnemius is also a powerful
flexor of that joint. However, it is not able to exert its full power on both
joints simultaneously. For example, if the knee is flexed, gastrocnemius cannot
exert maximum power at the ankle joint and vice versa.
Functional
activity
In running, walking and jumping gastrocnemius
provides a considerable amount of the propulsive force. When one considers the
power needed to throw the body into the air, triceps surae must be one of the
most powerful muscle groups in the body.
The habitual wearing of shoes with a high heel
can cause considerable shortening of the fibres of gastrocnemius, as the two
attachments of the muscle fibers are brought closer together. If shortening has
occurred, difficulty in walking in flat shoes or bare feet may be experienced
due to limited dorsiflexion at the ankle joint.

Soleus
This muscle is situated deep to gastrocnemius,
being a broad flat muscle wider in its middle section and narrower below
(figure b). It arises from the soleal
line on the posterior surface of
the tibia, the posterior surface of the upper
third of the fibula (including
the head) and a fibrous arch between these bony attachments. The fibres pass
downwards, forming a belly about half way down the calf to the deep surface of
a membranous tendon which faces posteriorly. This tendon glides over a similar
one on the deep surface of gastrocnemius, thereby enabling independent movement
of the two muscles to occur. Inferiorly the two tendons fuse to form the upper
part of the tendocalcaneus, which passes behind the ankle joint to insert into
the middle part of the posterior surface of the calcaneus.
Nerve
supply
Soleus is supplied by two branches from the tibial nerve, root value S1, 2, one
of which arises in the popliteal fossa and enters the superficial surface of
the muscle, while the other arises in the calf entering the deep surface. The
skin over the region of the muscle is predominantly supplied by root S2.
Action
Soleus is one of two main plantarflexors of the
ankle joint. It is so placed to prevent the body falling forwards at the ankle
joint during standing, and as such is an important postural muscle.
Intermittent contraction of the muscle during standing aids venous return(the
soleal pump) due to the communicating vessels joining the deep and superficial
venous systems which pass through its substance.
Plantaris
Plantaris(picture c) is a long, slender muscle
which is variable in its composition. It may have one muscle belly high up in
the calf, or two smaller bellies separated by a tendon. It arises from the
lowest part of the lateral supracondylar ridge, the adjacent part of the
popliteal surface of the femur and
the knee joint capsule. The tendon passes obliquely downwards between
gastrocnemius and soleus to emerge on the medial side of the tendocalcaneus. It
may insert into the tendocalcaneus or into the medial side of the posterior
surface of the calcaneus.
Nerve
supply
The supply to plantaris is from the tibial
nerve, root value S1, 2.
Action
Plantaris is a weak flexor of the knee and
plantarflexor of the ankle joint.
The tendocalcaneus (Achilles tendon)
This is considered to be the thickest and
strongest tendon in the body, being the tendon by which the calf muscles exert
their force on the posterior part of the foot during the propulsive phase of many activities, for example, walking,
running and jumping. It has been suggested that the tendocalcaneus is able to
withstand strains of up to 10 tons. As its fibres pass downwards they spiral
through some 90°, with the medial fibres passing posteriorly. This unusual
arrangement is thought to explain the apparent elastic qualities of the tendon.
For example, when jumping the body will land in an upright position with the foot held in plantarflexion by the
active triceps surae. The strain is then taken by the tendocalcaneus which
produces a recoil effect.
Functional
activity of the calf muscles
The action of the calf muscles as a whole is to
plantarflex the foot at the ankle
joint. Gastrocnemius acts as the propelling force, working mainly on the ankle
but also producing flexion of the knee if working strongly enough. The soleus,
on the other hand, is better situated to act more as a postural muscle. This is
because its lower attachment is the fixed point and prevents the leg from
falling forwards under the influence of body weight, because the vertical
projection from the centre of gravity of the body falls in front of the ankle
joint.
Gastrocnemius is composed of muscle fibres
which give it a pale appearance; consequently it is often referred to as
“white” muscle, whereas; the soleus has fibres which give it a red appearance
and is therefore termed a “red” muscle.
Plantaris takes very little in plantarflexion
of the ankle and, in fact, sometimes causes pain and disability when it is
torn. This condition is referred to as “tennis leg”, occurring during a game of
tennis, when the player believes that he or she has been struck on the back of
the calf by a tennis ball. The tendon is often completely ruptured and may have
to be surgically removed.
Palpation
of the calf muscles
When standing, draw your hand down the back of
the knee. The two large muscular bellies of gastrocnemius can be felt on either
side of the upper part of the calf. The medial head projects slightly higher
and lower than the lateral. Both can be felt joining a board flattened tendon
just over half way down the calf. The junction between the muscle fibres and
the tendon is very clear and it is along this line that many injuries of the
calf occur.
Soleus is not quite so easy to palpate being
deep to gastrocnemius, its lateral boundary appearing as a flattened elevation
below and lateral to the lateral head of gastrocnemius when the ankle is
plantarflexed. When standing on tiptoe, soleus can be seen and felt to bulge
either side of gastrocnemius. Passing the hand further down the calf it will
encounter the flattened tendocalcaneus, which is felt to narrow and become
rounded at the level of the ankle joint. It then expands slightly to its
insertion into the middle section of the posterior surface of the calcaneus.
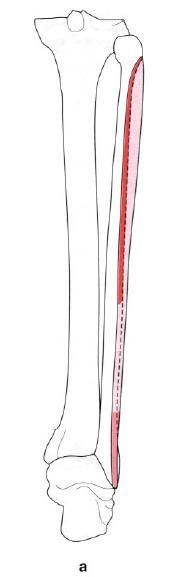
Peroneus longus
Peroneus longus(picture a) is situated on the
lateral side of the leg, being a long, thin fusiform muscle with a long belly
and an even longer tendon. It is also quite unique in as much as the tendon
changes direction three times on its way to its insertion on the medial side of
the sole of the foot.
It arises from a small area on the lateral condyle of the tibia( in conjunction with extensor digitorum longus) and the upper two-thirds of the lateral surface of the fibula, its lower half lying behind the upper part of the
origin from the lateral side of the head of the fibula, leaving a small area around the neck for the anterior
passage of the common peroneal nerve. In front and behind, it attaches to the
intermuscular septa and to the fascia surrounding the muscle.
The tendon forms about a hand’s breadth above
the lateral malleolus and lies superficial to that of peroneus brevis, sharing
the same synovial sheath. It runs in a shallow groove behind the lateral
malleolus passing deep to the superior peroneal retinaculum. From here, the
tendon passes downwards and slightly forwards to pass below the peroneal
tubercle on the calcaneus, being held in position by the inferior band of the
peroneal retinaculum. At this point the tendon is enclosed in a separate synovial
sheath. As it reaches the inferolateral side of the cuboid, which it grooves,
the tendon turns to enter the groove on the inferior aspect of the cuboid. This
groove is converted into a tunnel by fibres from the long plantar ligament and
tibialis posterior tendon, whilst in this tunnel the tendon is still surrounded
by a synovial sheath. The tunnel conveys the tendon forwards and medially
across the foot to its final
attachment to the plantar and lateral surfaces of the medial cuneiform and base of the first metatarsal.
Nerve
supply
Peroneus longus is supplied by the superficial peroneal nerve, root value
L5, S1. The skiin covering the muscle is supplied by L5, S1.
Action
The muscle is an obvious evertor of the foot because of the fact that it
arises from the lateral side of the leg and passes around the lateral side of the foot. In passing from behind the
lateral malleolus to the medial cuneiform and first metatarsal, peroneus longus
will produce plantarflexion of the foot,
with the medial side of the foot
being particularly drawn downwards, as in pronation.
It is worth noting that the insertion of this
muscle is to the same two bones as tibialis anterior, although the latter
muscle approaches its insertion from the medial side of the foot. This is believed to provide a stirrup for the arches of
the foot and help control their height during activity. The attachment of both
muscles to the medial cuneiform and base of the first metatarsal certainly
emphasizes the importance of control of the medial side of the foot in
activity, particularly when dealing with uneven terrain.
Functional
activity
In standing, peroneus longus, in company with
other surrounding muscles, helps to maintain the erect position. It controls
sideways sway by pressing the medial side of the foot on to the ground. This function is better seen and
appreciated when standing on one leg when peroneus longus works very hard to
maintain the leg over the foot and
prevent the body falling to the opposite side. Its main functional activity,
however, must be during powerful action of the foot as in running, particularly over rough ground. Here, its control,
together with that of tibialis anterior, over the medial side of the foot and the first
metatarsal(carrying the great toe), must be vital.
Palpation
When sitting, place the fingers on the lateral
side of the knee joint and locate the head of the fibula just below the joint level. The tendon of biceps femoris can be identified coming
from the back of the thigh. Run the fingers downwards, keeping the tip of the
index finger on the head of the fibula
spreading the rest of the finger tips down the lateral side of the fibula. Keeping the fingers in this
position, lift up the outer side of the foot. The long vertical belly can be felt contracting. If the fingers are
now taken down to the lateral malleolus and placed below and behind it and the
same manoeuvre is performed, the two tendons of peroneus longus and brevis can
be palpated and can be traced to the peroneal tubercle where they part, the
longus passing below and the brevis passing above.
Tibialis posterior
Tibialis posterior is the deepest muscle on the
back of the leg. It arises from the upper
half of the lateral aspect of the
posterior surface of the tibia below the soleal line, the interosseus membrane, the posterior surface of the fibula between the medial crest and
interosseus border, and the fascia covering it posteriorly. The tendon,
enclosed in its own synovial sheath, passes behind the medial malleolus
grooving it, being medial to flexor hallucis longus and flexor digitorum
longus. It lies superficial to the deltoid ligament. Lying inferior to the
plantar calcaneonavicular ligament, the tendon passes downward to attach
principally to the tubercle on the medial side of the navicular and the plantar
surface of the medial cuneiform.
Tendinous expansions pass to the plantar
surfaces of all the tarsal bones
except the talus, although a strip passes back to the tip of the sustentaculum tali, and the bases of the
middle three metatarsals.

Nerve
supply
Tibialis posterior is supplied by a branch of
the tibial nerve, root value L4, 5.
The skin over the area on the back of the calf is supplied by root S2.
Action
Tibialis posterior is the main invertor of the foot, acting in conjunction with
tibialis anterior. By its attachment to the tubercle of the navicular, it pulls
upwards and inwards and therefore rotates the forefoot so that the plantar
aspect faces medially. It must be noted that inversion and eversion of the foot
involve movement at the midtarsal joint, whereby the navicular and cuboid move
on the head of the talus and the calcaneus respectively.
The muscle is also a plantarflexor of the foot at the ankle joint, but its
contribution is small; gastrocnemius and soleus are better situated and have a
more direct line of action. Nevertheless, if the tendocalcaneus is ruptured,
then tibialis posterior can produce plantarflexion. Because of its attachments
to both the tibia and fibula, contraction of tibialis
posterior will tend to bring the two bones closer together. Consequently,
during plantarflexion, the malleoli are approximated to maintain their firm
grip on the narrower posterior part of the trochlear surface of the talus.
Functional
activity
Tibialis posterior will help to maintain the
balance of the tibia on the foot, particularly when body weight
is tending to move laterally. Being a strong invertor, it controls the forefoot
in walking and running by positioning the foot so that the medial arch is not completely flattened. Its many
tendinous expansions help to maintain all the various arches of the foot.
Palpation
It is quite impossible to palpate the belly of
the muscle due to the other muscles covering it. It is however quite easy to
feel the tendon of the muscle as it passes behind the medial malleolus and
particularly as it attaches to the tubercle of the navicular. When lying
supine, the tendon can be felt and seen behind the medial malleolus when
inversion of the plantarflexed foot against resistance is attempted. From just
above the flexor retinaculum to its insertion, it is surrounded by a synovial
sheath and it is in this area that the tendon can become quite painful if the
muscle has been overactive. The pain is sharp and knife-like and is termed
tenosynovitis.
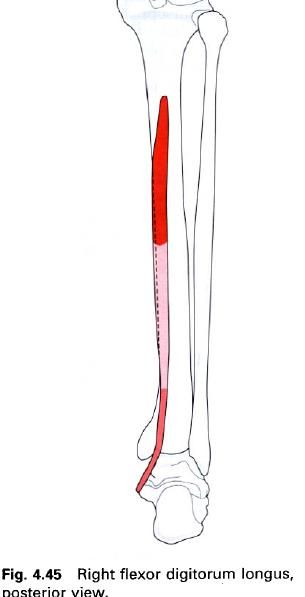
Flexor digitorum longus
Flexor digitorum longus is situated on the back
of the calf deep to soleus for most of its course. It arises from the medial part of the posterior surface of the tibia
below the soleal line, and from the deep transverse fascia surrounding it.
The tendon forms about three fingers’ breadth above the medial malleolus, lying
next to that of tibialis posterior, which has crossed anterior to it to come to
lie on its medial side, and medial to the tendon of extensor hallucis longus.
Passing deep to the flexor retinaculum the tendon lies in its own synovial
sheath along the medial aspect of the sustentaculum tali, sometimes grooving
it, to enter the sole of the foot
deep to abductor hallucis. Passing forwards and laterally, it crosses the tendon
of flexor hallucis longus (on its plantar aspect) and usually receives a slip
from that tendon which passes into the medial two of its four digitations.
About half way along the sole, on its lateral side, the tendon is joined by
flexor accessories(quadratus plantae) and at this point breaks up into its four
individual tendons; one for each of the lateral four toes. Just distal to the
attachment of flexor accessorius (quadratus plantae) the lumbrical muscles
arise.
Just distal to the metatarsophalangeal joint,
the tendons enter their respective fibrous sheaths, together with the
appropriate tendon of flexor digitorum brevis which lies superficial to it. The
tendon of brevis then splits to enable that of longus to pass through and reach
the plantar surface of the base of the distal phalanx where it inserts. Both
tendons share a common synovial sheath.
Nerve
supply
Flexor digitorum longus is supplied by the tibial nerve, root value L5, S1, 2. The
skin covering this area on the medial and posterior aspect of the calf and the
sole is supplied by roots L4, 5, S1.
Action
Flexor digitorum longus flexes the lateral four
toes. It flexes the distal interphalangeal joints first, then the proximal
interphalangeal joints and finally the metatarsophalangeal joints. Its course
behind the medial malleolus means that flexor digitorum longus also helps to
plantarflex the foot at the ankle joint. With the ankle plantarflexed, its
flexing action on the toes is diminished.
Functional
activity
In the propulsive phase of running, jumping or
walking, flexor digitorum longus pulls the toes firmly downwards towards the
ground to get the maximum grip and thrust during the toe-off phase. When the
body is in the standing position, the toes tend to grip the ground to improve
the balance.
Palpation
This muscle is very difficult to distinguish as
its origin is deep to soleus in the calf, while its tendons in the foot, with the lumbricals, lie
deeply. However, with care, the tendon can just be identified as it passes
alongside the sustentaculum tali.
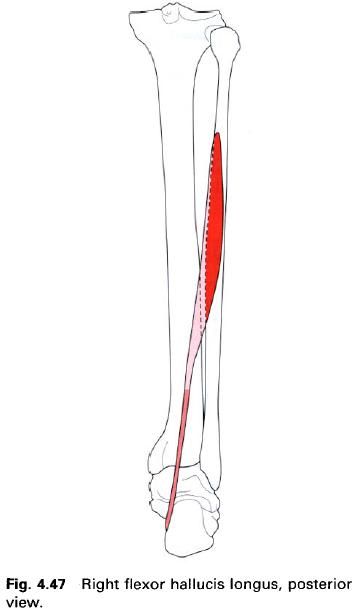
Flexor hallucis longus
Flexor hallucis longus is a powerful pinnate
muscle situated deep to triceps surae below the deep fascia of the calf. It
arises from the lower two-thirds of
the posterior surface of the fibula and from the adjacent fascia.
The muscle fibers pass to a central tendon
which lies on its superficial surface, with those on the lateral side extending
lower. The tendon passes downwards, deep to the flexor retinaculum in its own
synovial sheath, to cross the posterior aspect of the ankle joint lying lateral
to flexor digitorum longus. During its course, it grooves the lower end of the tibia, the back of the talus (between
the medial and posterior tubercles) and the inferior surface of the
sustentaculum tali, where it is held in position by a synovial-lined fibrous
sheath which forms a tunnel for it to run through.
In the sole of the foot, the tendon lies superficial to the plantar calcaneonavicular
ligament lying lateral to the tendon of the flexor digitorum longus. As it passes
forwards, the tendon of flexor hallucis longus crosses deep to that of flexor
digitorum longus, and in doing so usually gives a slip to its medial two
tendons. It then enters the fibrous digital sheath of the great toe, passing
between the two sesamoid bones situated on either side of the base of the
proximal phalanx, to insert into the plantar
surface of the base of the distal phalanx.
Nerve
supply
Flexor hallucis longus is supplied by a branch
of the tibial nerve, root value S1,
2. The skin covering this area is supplied by root S2.
Action
Flexor hallucis longus flexes all of the joints
of the great toe. It first acts on the interphalangeal joint and then the
metatarsophalangeal joint. As it crosses the ankle joint, it helps to produce
plantarflexion of the foot.
Functional
activity
Flexor hallucis longus is of great importance
in that it produces much of the final thrust from the foot during walking. At
this point in the gait cycle, the calf has already produced its maximum power
and the flexors of the lateral four toes are just completing their maximum
contraction. Flexion of the great toe is thus the final act before the foot is lifted from the ground ready
for the next step. It must also be remembered that the muscle is an important
factor in maintaining the medial longitudinal arch.
Palpation
Once again, flexor hallucis longus is almost
impossible to palpate as it lies deep to the calf muscles, flexor retinaculum,
plantar aponeurosis and the muscles in the foot.
Its tendon is set both deep within the calf and the plantar aspect of the foot.
4. 5. 2013.
Muscles medially rotating the tibia at the knee joint
Popliteus
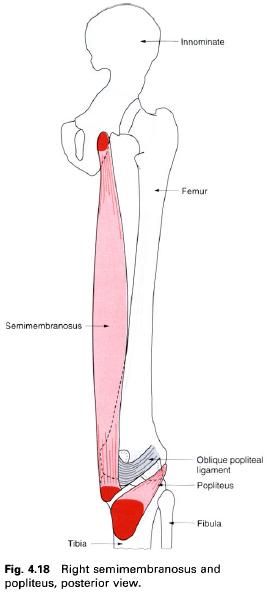
Popliteus
Popliteus is a triangularly shaped muscle
situated deep in the popliteal fossa, below and lateral to the knee joint. It
arises within the joint capsule from a tendinous attachment from the anterior
aspect of the groove on the outer surface of the lateral condyle of the femur,
below the lateral epicondyle and the attachment of the fibular collateral
ligament. The tendon passes backwards, downwards and medially, crossing the
line of the joint over the outer border of the lateral meniscus to which it is
attached. This upper part, within the capsule of the knee joint, is enveloped
in a double layer of synovial membrane until it leaves the capsule under the
arcuate popliteal ligament, from which it has a fleshy origin. Continuing
downwards and medially, popliteus attaches by fleshy fibres to a triangular
area on the posterior surface of the tibia above the soleal line, and the
fascia covering the muscle.
Nerve
supply
Popliteus is supplied by a branch from the
tibial division of the sciatic nerve,
root value L5, which enters the muscle on its anterior surface after winding
around its inferolateral border. The skin covering the area is supplied mainly
by S2.
Action
Popliteus laterally rotates the femur on the tibia when the foot is on
the ground, thus releasing the knee from its closepacked or locked position
allowing the knee to flex. By exerting a backward pull on the lateral surface
of the lateral condyle of the femur,
the condyle is rotated laterally about a vertical axis running through it just
medial to its centre. This allows the medial condyle of the femur to glide forward, releasing the
ligaments and muscles involved in its closepacked position.
When strong flexion of the knee is required,
popliteus comes into action, drawing the tibia
backwards on the femoral condyles, and if the foot is off the ground, it will aid the medial hamstrings in medial
rotation of the tibia.
Through its attachments to the lateral
meniscus, it pulls the meniscus backwards during lateral rotation of the femur, preventing it from being trapped
between the moving bones. This is believed by some authorities to be the reason
for the lateral meniscus being damaged much less frequently than the medial.
Пријавите се на:
Коментари (Atom)






