



Tibialis anterior
Extensor digitorum longus
Extensor hallucis longus
Peroneus tertius
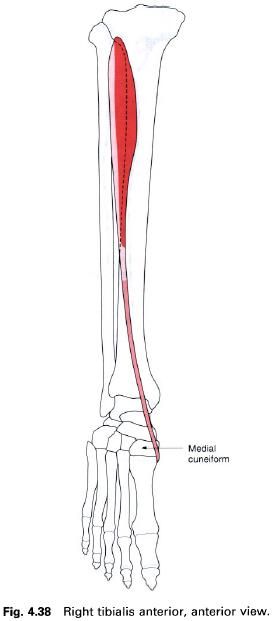
Tibialis anterior
Tibialis anterior is a long fusiform muscle
situated on the front of the leg lateral to the anterior border of the tibia. It is covered by strong fascia
and gains its upper attachment from the deep surface of this fascia, the upper two-thirds of the lateral surface of the tibia and the adjoining part of the interosseus membrane. The muscle becomes
tendinous in its lower third, passing downwards and medially over the distal
end of the tibia. The tendon
continues through both the superior and inferior extensor retinaculae to insert
into the medial side of the medial cuneiform and base of the first metatarsal, the insertion reaching the under surface of both
bones to blend with that of peroneus longus.
Nerve
supply
This muscle is supplied by the deep peroneal nerve, root value L4, 5.
The skin covering the muscle is also supplied by roots L4, 5.
Action
Tibialis anterior is a dorsiflexor of the foot at the ankle joint. When working
with tibialis posterior it acts as an
invertor of the foot, in which the
sole of the foot is turned to face
medially.
Functional
activity
As with other muscles in the leg, tibialis
anterior is concerned with balancing the body on the foot. It works with the surrounding muscles to maintain body
balance during activities of the upper part of the body which change the
distribution of weight.
Not only is tibialis anterior responsible for
dorsiflexing the foot as the lower
limb is carried forward during the swing-through phase of walking, so
preventing the toes catching the ground, it also controls the placement of the foot on the ground following initial
ground contact by the heel. On close observation, especially in slow motion, it
will be seen that the heel does not strike the ground and remain immobile at
the initiation of the stance phase, but glides on to the surface and acts as
the first braking force of the lower limb’s forward movement. Overactivity of
tibialis anterior accounts for the wear patterns seen on the posterolateral
aspect of the heel, due to the frictional forces between the shoe and the
ground. The rest of the foot is then
gradually lowered to the ground in a controlled manner taking up the
undulations of the surface concerned. The landing of the foot on the ground is similar to the landing of an aeroplane; the
main wheels touch down first applying the initial braking force followed by a
controlled lowering of the front of the craft as the speed decreases.
Tibialis anterior in association with the other
dorsiflexors, therefore, plays an important part in the lowering of the
forefoot to the ground in walking or running and will be put under stress in
extended activity particularly over rough terrain. The anterior calf muscles
are enclosed in particularly tight fascia which allows very little expansion of
the tissues. The result is a compression of the muscle during activity and a
dragging on the attachments of the surrounding fascia, particularly where it
attaches to the bone. This leads to a painful condition of this area commonly
called “shin splints”.
Paralysis of tibialis anterior causes footdrop
because the remaining dorsiflexors are not strong enough to raise the toes and
so prevent them dragging along the ground. The patient may overcome this by
flexing the knee more than normal during walking or by fitting a “toe-raise”
orthosis to patients or their shoe.
Palpation
Both the muscle belly and tendon can be seen
and felt when the foot is dorsiflexed
against resistance, the tendon being the most medial at the ankle joint.
Extensor digitorum longus
Extensor digitorum longus is again situated on
the anterior aspect of the leg, being lateral to tibialis anterior, and
overlying extensor hallucis longus. It has a linear origin from the upper-two thirds of the anterior surface of the fibula, the deep fascia and the upper
part of the interosseus membrane with its upper fibres reaching across the lateral condyle of the tibia in conjunction with those of peroneus longus. It is a pennate muscle
with the tendon appearing on the medial side; the muscle fibres pass downwards
and medially to reach it. The tendon passes over the front of the ankle joint
deep to the superior extensor retinaculum and then through the loop of inferior
extensor retinaculum accompanied by peroneus tertius. At the level of the
inferior extensor retinaculum or immediately distal, it gives rise to four
tendons which run to the lateral four toes. The four separate tendons are
enclosed in a common synovial sheath at the level of the inferior extensor
retinaculum. On the dorsal surface of the proximal phalanx, each tendon forms a
triangular membranous expansion, known as the extensor hood (dorsal digital expansion). Each hood is joined on
its medial side by the tendon of the lumbrical and on the lateral side for the
second to fourth toes by the tendon of extensor digitorum brevis. The
interossei of the foot do not have an attachment to the extensor hood.
As the hood passes forwards over the proximal
phalanx it divides into three parts before reaching the dorsum of the proximal
interphalangeal joint. The central portion attaches to the base of the middle phalanx, while the two outer
portions unite before inserting on to the base of the distal phalanx. An attachment of the extensor hood to the dorsal
aspect of the proximal phalanx has also been described.
Nerve
supply
This muscle is supplied by the deep peroneal nerve, root value L5, S1.
The skin covering the muscle is supplied by root L5.

Action
As its name implies, extensor digitorum longs
is an extensor of the lateral four toes at the metatarsophalangeal joints, and
also assists in extension at the interphalangeal joints. However it is unable
to perform the latter action unaided, which is primarily performed by the
lumbricals. If the lumbricals are paralysed, extensor digitorum longus produces
hyperextension of the metatarsophalangeal joint, while the interphalangeal
joints become flexed. As the muscle passes across the front of the ankle joint,
it also aids in dorsiflexion of the foot.
Functional
activity
During walking and running extensor digitorum
longus draws the toes upwards after they have been flexed prior to toe-off, and
keeps them clear of the ground until the heel and foot make contact with the
ground again. Unfortunately, the lateral four toes in most individuals tend to
be flexed at the proximal interphalangeal joint and extended at the distal
interphalangeal joint. Consequently extensor digitorum longus will lift the
toes in this adapted position.
Palpation
The muscle belly is easily palpated on the
anterolateral aspect of the leg. From the head of the fibula on the lateral side of the leg, just below the knee joint,
run the fingers downwards and medially for about 2cm. When raising the toes off
the floor, the muscle can be felt contracting. Now place the fingers over the
front of the ankle joint; the tendon can be identified standing out clearly,
being lateral to those of tibialis anterior and extensor hallucis longus. From
here the tendon can now either be traced upwards, under the superior part of
the extensor retinaculum to join the muscle belly, or downwards where it breaks
up into four individual tendons running towards each of the lateral four toes.
Each tendon stands clear of the metatarsophalangeal joint as it passes towards
the dorsum of the toe.
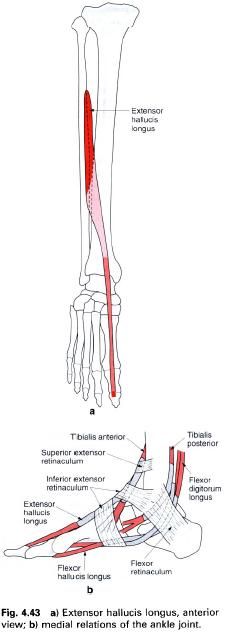
Extensor hallucis longus
Extensor hallucis longus is situated deep to
and between tibialis anterior and extensor digitorum longus on the front of the
leg. Arising from the middle half of
the anterior surface of the fibula and the adjacent interosseus membrane, the muscle fibres
pass downwards and medially to the tendon which forms on its anterior surface.
In this respect it is a unipennate muscle. The tendon passes under the superior
extensor retinaculum, through the upper part of the inferior extensor
retinaculum in a separate compartment enclosed in its own synovial sheath, and
then deep to the lower band of the inferior extensor retinaculum on its way
towards the base of the great toe. Generally, the tendon does not form a fully
developed extensor hood but passes to attach to the base of the distal phalanx
on its dorsal surface. Tendinous slips may be given off to the dorsal aspect of
the base of the proximal phalanx and the first metatarsal.
Nerve
supply
Extensor hallucis longus is supplied by the deep peroneal nerve, root value L5, S1.
The skin covering this area is supplied by roots L4, 5.
Action
As its name implies, extensor hallucis longus
will extend all of the joints of the great toe, but mainly the
metatarsophalangeal joint. It is also a powerful dorsiflexor of the foot at the ankle joint.
Functional
activity
In running, the great toe is the last part of
the foot to leave the ground and therefore the final thrust will come from the
long flexors of the toes. After this, the toe must be brought back into the
extended position at the same time as the foot
is dorsiflexed and slightly inverted, ready for the heel to be placed on the
ground for the next weightbearing phase. By extending the great toe and
dorsiflexing the foot, clearance of
the surface is also achieved. It should be noted that the great toe does not
have a lumbrical muscle or interossei associated with it. Consequently, extension
of the interphalangeal joint depends entirely on extensor hallucis longus.
Paralysis of the muscle will result in flexion of the joint and buckling of the
toe during the last phase of gait, due to the unopposed action of the flexor
muscles.
Palpation
If the great toe is extended, the tendon of the
muscle is clearly visible as it crosses the first metatarsophalangeal joint to
its insertion into the base of the distal phalanx. Trace the fingers up the
tendon; it can be felt and seen crossing the anterior aspect of the ankle joint
lateral to the tendon of tibialis anterior. From here the tendon can be felt
passing upwards and laterally before passing deep to the surrounding muscles.
Continue to move the fingers upwards for another 12cm and allow them pass a
little laterally; when the great toe is rhythmically extended and flexed, the
muscle can just be felt contracting under the fingers.
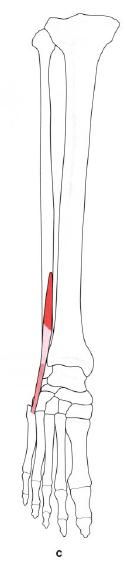
Peroneus tertius
Peroneus tertius is situated on the lower
lateral aspect of the leg and appears to have been part of extensor digitorum
longus. It arises from the front of
the lower quarter of the fibula in
continuation with the attachment of extensor digitorum longus (with no gap
between them), and from the intermuscular septum and adjoining fascia. Its
fibres pass downwards and laterally into a tendon which passes deep to the
superior and through the inferior extensor retinacula to insert into the medial
and dorsal aspect of the base of the fifth metatarsal.
Nerve
supply
Peroneus tertius is supplied by the deep peroneal nerve, root value L5, S1.
The area of skin covering the muscle is also supplied by roots L5, S1.
Action
The muscle acts as a weak evertor and
dorsiflexor of the foot at the ankle
joint.
Functional
activity
It is difficult to assess the importance of
this small muscle as its actions appear to be covered by other muscles which
have a much better mechanical leverage. Indeed in some subjects it is absent.
It does, however, pass over the anterior talofibular ligament of the ankle
joint, and it is well-known that this is very often damaged in inversion
injuries. It is therefore well placed to help prevent too much inversion during
sports activities, for example, and may be responsible for keeping down the
number of injuries. Unfortunately, the muscle is often torn and may be
completely ruptured during violent inversion, which is the cause of
considerable pain and swelling. It is possible that with the attainment of
bidepalism, peroneus tertius is assuming a more important role because eversion
of the foot is a peculiarly human
characteristic.
Palpation
Peroneus tertius is very difficult to palpate.
However, it can be felt by drawing the fingers downwards from the anterior part
of the lateral malleolus into the small hollow found there. The tendon can be
felt crossing the lateral part of the hollow to its insertion into the medial
side of the base of the fifth metatarsal. Take care not to confuse the tendon
of peroneus tertius with that of peroneus brevis, which lies lateral to this
point as it passes forwards to insert into the tubercle on the lateral side of
the fifth metatarsal.







0 коментара:
Постави коментар