



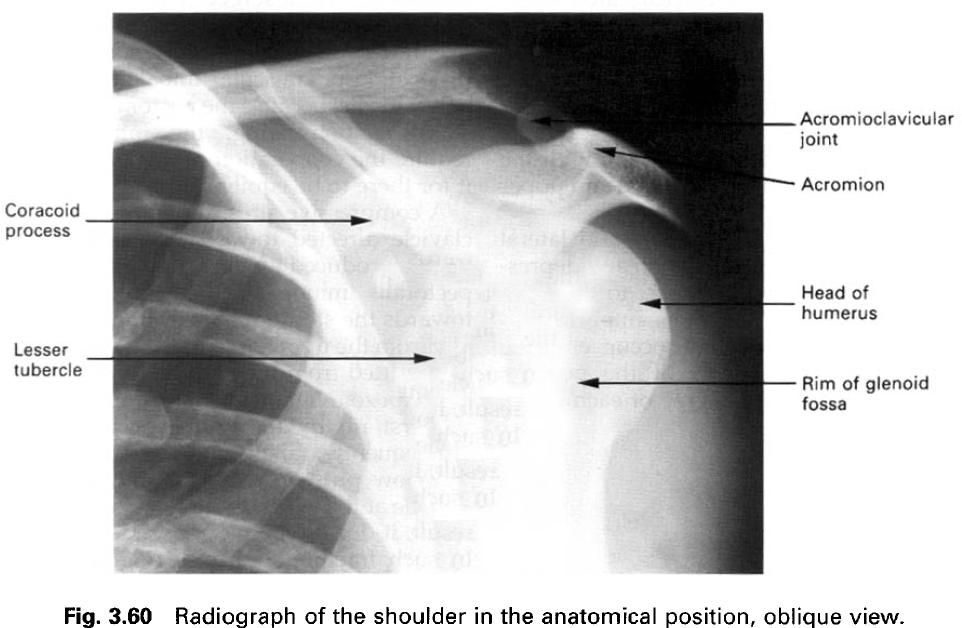
Introduction
The shoulder(glenohumeral) joint is the
articulation between the head of the humerus
and the glenoid fossa of the scapula.
The intrascapular presence of the epiphyseal line between the ventral coracoid
and dorsal scapula in the upper part
of the glenoid fossa facilitates adjustments of the joint surfaces during
growth of the bone. Similar arrangements are also to be found in the hip and
the elbow joints.
It is a synovial joint of the ball and socket
variety, with the head of the humerus
forming the ball and the glenoid fossa of the socket, in which freedom of
movement has been developed at the expense of the stability. The mobility of
the upper limbs from locomotor activity, and partly due to mobility of the
pectoral girdle linking the limb to the trunk. Comparison of the shoulder and
hip joints, equivalent joints in the upper and lower limbs, together with their
mode of attachment to the axial skeleton, reveals significant and important
differences between them even though the basic features of each are similar.
In the frontal plane, the axis of the head and
neck of the humerus forms an angle of
135° to 140° with the long axis of the shaft; this is the angle of inclination.
Because of this angulation, the centre of the humeral head lies about 1cm
medial to the long axis. Although the anatomical and mechanical axes of the humerus do not exactly coincide, unlike
the femur they both lie inside the bone(a). Consequently, the action of muscle
groups producing movement at the shoulder joint, especially that of medial and
lateral rotation, is more easily understood.

As well as being set at an angle to the shaft
of the humerus, the axis of the head
and neck is rotated backwards against the shaft some 30° to 40°; this is the
angle of retroversion(b). The magnitude of the angle of retroversion is said to
vary both with age and with race. It is thought that this angle has increased
with the attainment of bipedalism, in which there has also been flattening of
the thoracic cage anteroposteriorly, and a backward displacement of the scapula, the result being that as the
glenoid fossa came to be directed more laterally, the head and neck of the humerus became more twisted in an
attempt to maintain maximum joint contact between the two articulating bones.
Structurally this adaptation was not entirely successful, which to some extent
was fortuitous for in humans the use of the upper limb gradually changed from
one of support to one of manipulation.
Articular surfaces
The articular surfaces of the joint are the
rounded head of the humerus and the
rather shallow glenoid fossa. The adaptation of these two surfaces contributes
very little, if at all, to the stability and security of the joint. As in the
majority of synovial joints, the two articular surfaces are covered by hyaline
cartilage.
Glenoid fossa
The glenoid fossa is situated at the
superolateral angle of the scapula
and faces laterally, anteriorly and slightly superiorly. It is pear-shaped in
outline, with a narrower region superiorly, and concave both vertically and
transversely(a). However, the concavity of the joint is irregular and less deep
than the convexity of the head of the humerus.
In the plane of the axis of the head and neck of the humerus it has been estimated that the curvature of the glenoid
fossa, with its larger radius, subtends an angle of some 75°. The articular
surface of the fossa is little more than one-third of that of the humeral head.
It is deepened to some extent by the presence of the glenoid labrum.
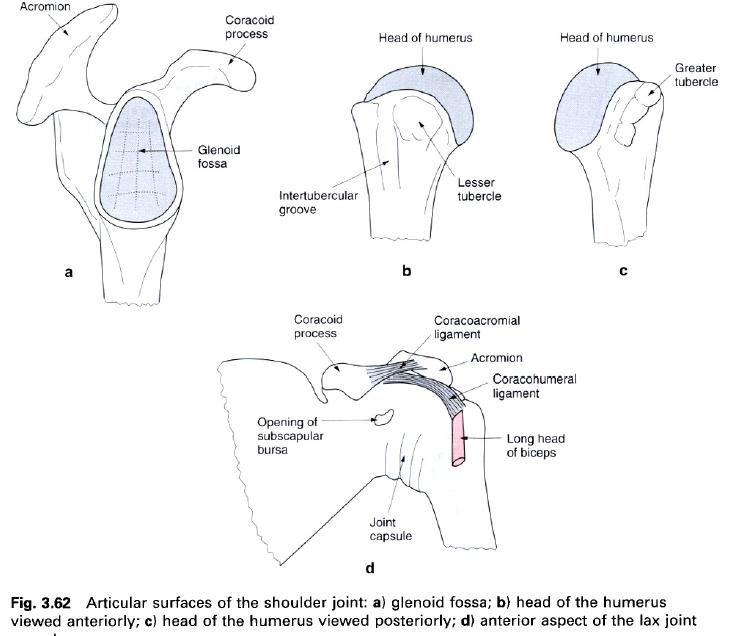
Head of the humerus
The head of the humerus represents two-fifths
of a sphere and faces superiorly, medially and posteriorly(b,c). With its
smaller radius of curvature, the articular surface subtends an angle of
approximately 150° in the plane of the axis of the head and neck. Regardless of
the position of the joint, only one-third of the humeral head is in contact
with the glenoid fossa at any time. It is essentially the mismatch in
coaptation of the articular surfaces which give the joint its mobility.
Joint capsule and synovial membrane
The fibrous capsule of the joint forms a loose
cylindrical sleeve between the two bones(d). The majority of the capsular
fibres pass horizontally between scapula
and humerus, but some oblique and
transverse fibres are also present. Although it is thick and strong in parts,
particularly anteriorly, because of its laxness the capsule conveys little
stability to the joint. On the scapula,
the capsule attaches just outside the glenoid labrum anteriorly and inferiorly,
and to the labrum superiorly and posteriorly. Recesses formed between the
anterior capsular attachment and the glenoid labrum may have pathological
significance in shoulder joint trauma.
On the humerus,
the capsule attaches to the anatomical neck, around the articular margins of
the head, medial to the greater and lesser tubercles, except inferiorly where
it joins the medial surface of the shaft about 1cm below the articular
margin(d). The dipping down of the capsular attachment medially causes the
medial end of the upper epiphyseal line of the humerus to become intracapsular.
The anterior part of the capsule is thickened
and strengthened by the presence of the three glenohumeral ligaments, which can
only be seen on its inner aspect. The superoposterior part is strengthened near
its humeral attachment by the coracohumeral ligament. The tendons of the
“rotator cuff” muscles spread out over the capsule; blending with it near their
humeral attachments. These short scapular muscles act as extensible ligaments,
and are extremely important in maintaining the integrity of the joint.
With the arm hanging in the anatomical
position, the lower part of the joint capsule is lax and forms a redundant
fold. When the arm is abducted this part of the capsule becomes increasingly
taut.
There are two openings in the fibrous capsule;
occasionally a third may be present. One is the upper end of the
intertubercular groove to allow the long head of biceps to pass into the arm(d). This part of the capsule is
thickened, forming the transverse humeral ligament, arching over the tendon as
it emerges from the capsule. The second opening is in the front of the capsule,
between the superior and middle glenohumeral ligaments, and communicates with
the subscapular bursa deep to the tendon of subscapularis(d).
A third communication of the joint cavity with the infraspinatus bursa.
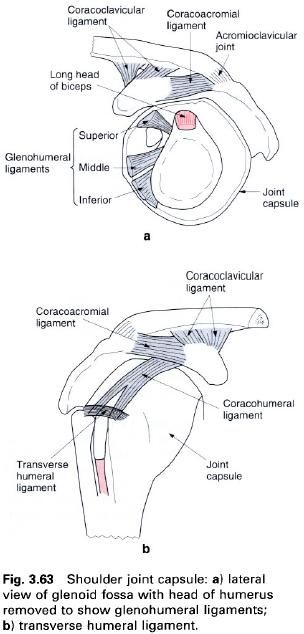
Capsular ligaments
The anterior part of the joint capsule is
reinforced by three longitudinal bands of fibres called the glenohumeral
ligaments(a). They are seldom prominent and when present radiate from the
anterior glenoid margin extending downwards from the supraglenoid tubercle.
Superior
glenohumeral ligament. The
slender superior glenohumeral ligament arises from the upper part of the
glenoid margin and adjacent labrum immediately anterior to the attachment of
the tendon of the long head of biceps.
It runs laterally parallel to the biceps
tendon to the upper surface of the lesser tubercle.
Middle
glenohumeral ligament. The
middle glenohumeral ligament arises below the superior and attaches to the humerus on the front of the lesser
tubercle below the insertion of subscapularis.
Inferior
glenohumeral ligament. The
inferior glenohumeral ligament is usually the best developed of the three
ligaments, although it is tend to increase the tension in some or all of the
glenohumeral ligaments. Lateral rotation of the humerus will put all three ligaments under tension, whereas medial
rotation relaxes them.
In abduction, only the middle and inferior
ligaments become taut, while the superior becomes relaxed.
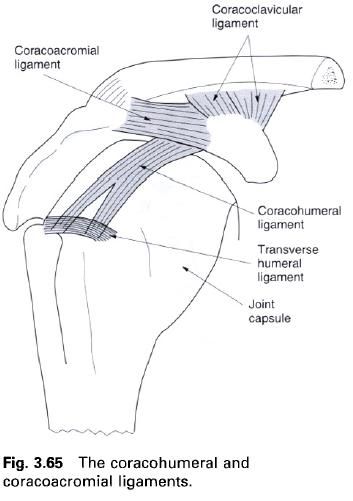
Transverse
humeral ligament. At the upper
end of the intertubercular groove, the transverse humeral ligament bridges the
gap between the greater and lesser tubercles(b). It is formed by some of the
transverse fibres of the capsule and serves to hold the biceps tendon in the intertubercular groove as it leaves the joint.
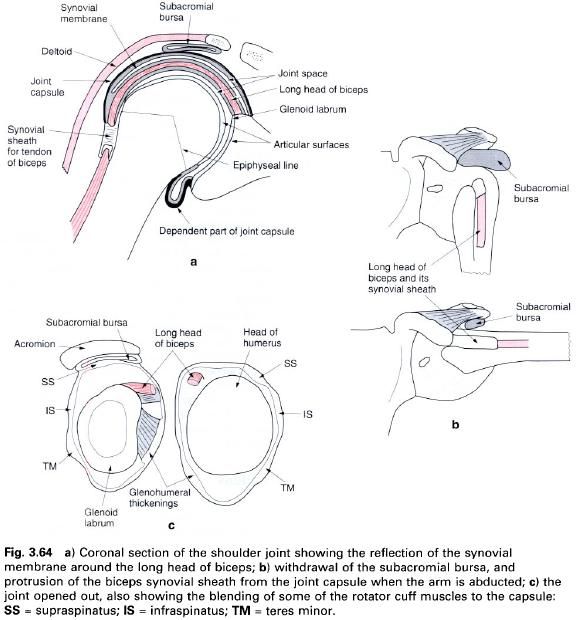
Synovial membrane
The synovial membrane of the joint lines the
capsule, and thus also extends downwards as a pouch when the arm is hanging by
the side(a). It attaches to the articular margins of both bones, and is
therefore reflected upwards on the medial side of the humeral shaft to its
attachment. Consequently, although the medial part of the epiphyseal line is
intracapsular, it is extrasynovial(a). The membrane extends through the
anterior opening of the capsule forming the subscapularis bursa, which may be
limited in its extent to the posterior surface of the tendon of subscapularis. However, it may be
sufficiently large to extend above the upper border of the tendon and so come
to lie below the coracoid process. This upward extension may be replaced by a
separate subcoracoid bursa. The posterior extension of the membrane through the
joint capsule forms the infraspinatus bursa.
The intracapsular part of the long head of biceps is enclosed within a
double-layered tubular sheath of synovial membrane which is continuous with
that of the joint at its glenoid attachment(a). This sheath surrounds the
biceps tendon as it passes beneath the transverse humeral ligament into the
intertubercular groove, and extends some 2cm into the arm(b).
An important, but non-communicating, bursa
associated with the shoulder joint is the subacromial bursa. It lies between,
and separates, the coracoacromial arch and deltoid from the superolateral part
of the shoulder joint. That part of the bursa which extends laterally under
deltoid is usually referred to as the subdeltoid bursa.
Some of these bursae are of clinical
significance as adhesions may form preventing free gliding movements. This is
particularly true for bicipital sheath and the subdeltoid bursa. Indeed, the
subdeltoid bursa may become inflamed(bursitis) and affect the underlying tendon
of supraspinatus, leading to its rupture in a small number of cases.
Intra-articular structures
Glenoid labrum
As in the hip joint, the glenoid fossa is
deepened by the presence of a fibrocartilaginous rim, the glenoid labrum(c). It
is triangular in cross-section, with a thin free edge and is about 4mm deep.
The base of the labrum attaches to the margin of the glenoid fossa; the outer
surface gives attachment to the joint capsule posteriorly and superiorly, while
the inner(joint) surface is in contact with the head of the humerus and is lined by cartilage
continuous with that of the glenoid fossa. The upper part of the labrum may not
be completely fixed to the bone so that its inner edge may project into the
joint like a meniscus.
The superior outer margin of the labrum gives
attachment to the tendon of the long head of biceps, while inferiorly the tendon of the long head of triceps partly arises from it.
Long head of biceps
The tendon of the long head of biceps runs intracapsularly from its attachment to
the supraglenoid tubercle and adjacent superior margin of the glenoid labrum until
it emerges from the joint deep to the transverse humeral ligament. During its
intracapsular course, and for some 2cm beyond, the tendon is ensheathed in a
synovial sleeve.
Accessory ligaments
Apart from the capsular ligaments, there are
two further ligaments associated with the shoulder joint. Both are considered
to be accessory ligaments, although one, the coracohumeral ligament, blends
with the joint capsule.
The other, the coracoacromial ligament,
completes a fibro-osseous arch above the joint.
Coracohumeral ligament
The coracohumeral ligament is a fairly strong,
broad band arising from the lateral border of the coracoid process near its
root. It becomes flattened as it passes laterally with its two margins
diverging above the intertubercular groove to attach to the upper part of the
anatomical neck in the region of the greater and lesser tubercles and to the
intervening transverse humeral ligament.
The anterior border of the medial part of the
ligament is free, but as it passes laterally it fuses with the tendon of subscapularis as it blends with the
capsule prior to its insertion on the lesser tubercle. The posterior part of
the ligament blends with the tendon of supraspinatus
as it attaches to the superior facet on the greater tubercle.
Coracoacromial ligament
The coracoacromial ligament is not directly
associated with the joint but forms, with the coracoid and acromion process, a
fibro-osseous arch above the head of the humerus.
It is a strong, triangular ligament, whose anterior and posterior borders tend
to be thicker than the intermediate part. Occasionally, the pectoralis minor tendon is prolonged and
pierces the base of the ligaments to become continuous with the coracohumeral
ligament. The coracoacromial ligament is attached by a broad base to the
lateral border of the horizontal part of the coracoid process, with the blunt
apex fixed to the apex of the acromion in front of the acromioclavicular joint.
Superiorly are the clavicle and deltoid, while inferiorly it is
separated from the tendon of the supraspinatus
and the shoulder joint by the subacromial bursa.





0 коментара:
Постави коментар