



Athletes experience various levels of fatique
during repeated days and weeks of training, so not all fatique-producing
situations can be classified as overtraining(as it is noted previously with
overreaching). Fatique that follows one or more exhaustive training sessions
usually is relieved by a few days of reduced training or rest and a
carbohydrate-rich diet. Overtraining, on the other hand, is characterized by a
sudden decline in performance and physiological function that cannot be
remedied by a few days of reduced training, rest, or dietary manipulation.
Effects of overtraining: the overtraining syndrome
Most of the symptoms that result from
overtraining, collectively reffered to as the overtraining syndrome, are
subjective and identifiable only after the individual’s performance and
physiological function have suffered. Unfortunately, these symptoms can be
highly individualized, making it very difficult for athletes, trainers, and
coaches to recognize that performance decrements are brought on by
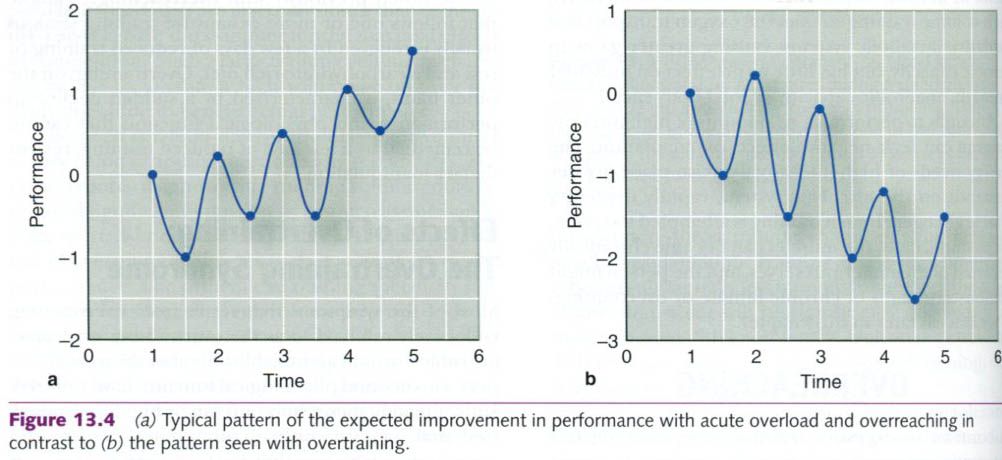
overtraining. A decline in physical performance with continued training is
usually the first indication of the overtraining syndrome(see figure below).
The athlete senses a loss of muscular strength, coordination, and working
capacity and generally feels fatiqued. Other primary signs and symptoms of
the overtraining syndrome include:
- Change in appetite;
- Body weight loss;
- Sleep disturbances;
- Irritability, restlessness,
excitability, anxiousness;
- Lack of mental
concentration;
- Feelings of depression;
- Lack of appreciation for
things that normally are enjoyable.
Physiological changes also indicate the
presence of the overtraining syndrome.
The underlying causes of overtraining syndrome
are often a complex combination of emotional and physiological factors. Hans
Selye noted that a person’s stress tolerance can break down as often from a
sudden increase in anxiety as from an increase in physical distress. The
emotional demands of competition, the desire to win, the fear of failure,
unrealistically high goals, and others’ expectations can be sources of
intolerable emotional stress. Because of this, overtraining is typically
accompanied by a loss of competitive desire and a loss of enthusiasm for
training. Furthermore, Armstrong and VanHeest make the important observation
that the overtraining syndrome and clinical depression involve remarkably
similar signs and symptoms, brain structures, neurotransmitters, endocrine
pathways, and immune responses, suggesting that they have similar etiologies.
The physiological factors responsible for the
detrimental effects of overtraining are not fully understood. However, abnormal
responses have been reported that suggest that overtraining is associated with
alterations in the nervous, endocrine, and immune systems. Although a
cause-and-effect relationship between these changes and the symptoms of
overtraining has not been clearly established, these symptoms can help
determine whether an individual is overtrained. In the following discussion, we
focus on some of the observed changes associated with overtraining and on
potential causes of the overtraining syndrome.
Autonomic
nervous system responses to overtraining
Some studies suggest that overtraining is
associated with abnormal responses in the autonomic nervous system.
Physiological symptoms accompanying the decline in performance often reflect
changes in those organs or systems that are controlled by either the
sympathetic or parasympathetic branches of the autonomic nervous system. Sympathetic
overtraining lead to:
- Increased resting heart rate;
- Increased blood pressure;
- Loss of appetite;
- Decreased body mass;
- Sleep disturbances;
- Emotional instability;
- Elevated basal metabolic
rate.
This form of overtraining occurs predominantly
among athletes who emphasize highly intense or resistance training methods.
Other studies suggest that the parasympathetic
nervous system might be dominant in some cases of overtraining, usually in
endurance athletes. In these cases, the performance decrements markedly differ
from those associated with sympathetic overtraining. Signs of
parasympathetic overtraining, assumed to be the result of volume overload,
include:
- Early onset of fatique;
- Decreased resting heart rate;
- Rapid heart rate recovery
after exercise;
- Decreased resting blood
pressure.
Thus, it appears that athletes in different
sports or events will likely exhibit unique signs and symptoms of overtraining
syndrome that are related to their training regimens. In fact, some authorities
have named these forms of overtraining “intensity related” and “volume
related”, recognizing that specific training stressors result in unique signs
and symptoms when applied excessively.
Some of the symptoms associated with autonomic
nervous system overtraining are also seen in people who are not overtrained.
For this reason, we cannot always assume that the presence of these symptoms
confirms overtraining. Of the two conditions, symptoms of sympathetic
overtraining are the most frequently observed. Although there is not strong
scientific evidence to support the autonomic nervous system overtraining
theory, the autonomic nervous system definitely is affected by overtraining.
Hormonal responses to overtraining
Measurements of various blood hormone
concentrations during periods of overreaching suggest that marked disturbances
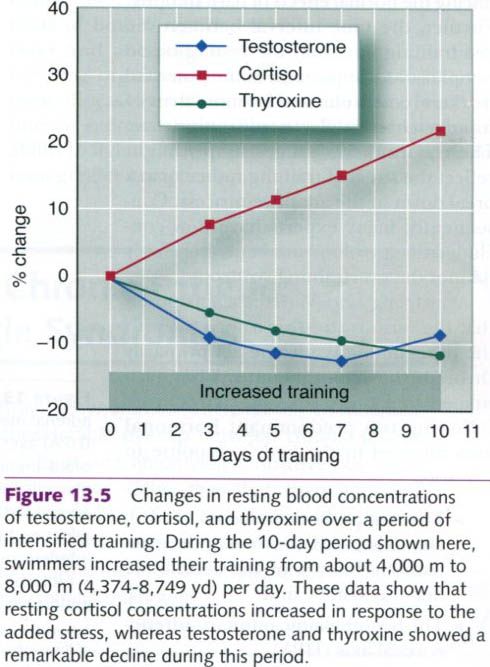
in endocrine function accompany excessive stress. As shown in the figure below,
when swimmers increase their training 1.5-to-2-fold, blood concentrations of
thyroxine and testosterone usually decrease and blood concentrations of
cortisol increase. The ratio of testosterone to cortisol is thought to regulate
anabolic processes in recovery, so a change in this ratio is considered an
important indicator, and perhaps a cause, of the overtraining syndrome.
Further, most overtraining studies have been conducted on aerobically trained
endurance athletes. Fewer studies exist on anaerobically trained and
resistance-trained athletes. Using the terminology introduced in the last
section, intensity-related overtraining(anaerobic and resistance training) does
not appear to alter resting hormonal concentrations.
Overtrained athletes often have higher blood
concentrations of urea, and because urea is produced by the breakdown of
protein, this indicates increased protein catabolism. This mechanism is thought
to be responsible for the loss in body mass seen in overtrained athletes.
Resting blood concentrations of epinephrine and norepinephrine have also been reported to be elevated during periods of
intensified aerobic or volume training. These two hormones elevate heart rate
and blood pressure. This has led some exercise physiologists to suggest that
the blood concentrations of these catecholamines should be measured to confirm overtraining.
However, other studies have found no change in these catecholamines during
intensified training, and some have even found decreased resting values.
Acute overload training and overreaching often
produce most of the same hormonal changes reported in overtrained athletes. For
this reason, measuring these and other hormones might not provide valid
confirmation of overtraining. Athletes whose hormone concentrations appear
abnormal may simply be experiencing the normal effects of hard training. Further,
the time interval between the last training bout and the resting blood sample
is very important. Some potential markers remain elevated for more than 24h and
might not reflect a true resting state. These hormonal changes simply might
reflect the stress of training rather than a breakdown in the adaptative
process. Consequently, many experts have now concluded that no blood marker
conclusively defines the overtraining syndrome.
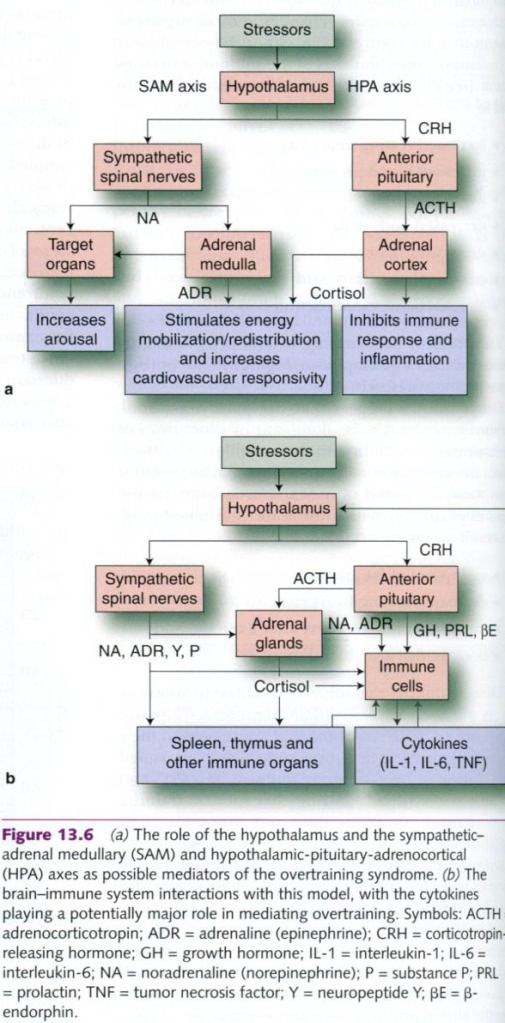
Armstrong and VanHeest proposed that the
various stressors associated with the overtraining syndrome act primarily
through the hypothalamus. They postulated that these stressors activate the
following two predominant hormonal axes involved in the body’s response to
stressors:
- The sympathetic-adrenal
medullary axis(SAM), involving the sympathetic branch of the autonomic
nervous system;
- The
hypothalamic-pituitary-adrenocortical axis(HPA).
This is illustrated in the picture a below.
Figure b illustrates the brain and immune system interactions with these two
axes. These two figures are quite complex and go well beyond the scope of an
introductory-level exercise physiology text. However, a cursory study of the
interactions depicted in these figures will give an appreciation of the
complexity of this syndrome. Importantly, note that the stressors have their
initial effect on the brain(hypothalamus). Thus, it is highly likely that brain
neurotransmitters play an important role in the overtraining syndrome.
Serotonin is a major neurotransmitter that is suspected to play a significant
role in the overtraining syndrome. Unfortunately, plasma concentrations of this
important neurotransmitter do not accurately reflect those concentrations in
brain. Advances in techonology should provide the necessary tools to help us
better understand what is going on inside the brain.
A major role for cytokines in the overtraining
syndrome, recently has been proposed, providing support for the Armstrong and
VanHeest model in figure b. Elevated circulating cytokines result from
infection as well as from skeletal muscle, bone, and joint trauma associated
with overtraining. They appear to be a normal part of the body’s inflammatory
response to infection and injury. It is theorized that excessive
musculoskeletal stress, coupled with insufficient rest and recovery, sets up a
cascade of events whereby a local acute inflammatory response evolves into
chronic inflammation and eventually into systemic inflammation. Systemic
inflammation activates circulating monocytes, which can then synthetize large
quantities of cytokines. Cytokines then act on most of the brain and body
functions in a manner consistent with symptoms expressed in the overtraining
syndrome.
Immunity and overtraining
The immune system provides a line of defense
against invading bacteria, parasites, viruses, and tumor cells. This system
depends on the actions of specialized cells(such as lymphocytes, granulocytes,
and macrophages) and antibodies. These primarily eliminate or neutralize
foreign invaders that might cause illness(pathogens). Unfortunately, one of the
most serious consequences of overtraining is the negative effect it has on the
body’s immune system. In fact, from the model proposed in the figure above,
compromised immune function is potentially a major factor in the initiation of
the overtraining syndrome.
Many studies have shown that excessive training
suppresses normal immune function,
increasing the overtrained athlete’s susceptibility to infections. This is
illustrated in the picture below. Studies also show that short bouts of intense
exercise can temporarily impair the immune response, and successive days of
heavy training can amplify this suppression. Several investigators have
reported an increased incidence of illness following a single, exhaustive
exercise bout, such as running a full 42km(26.2 mi) marathon. This immune
suppression is characterized by abnormally low concentrations of both
lymphocytes and antibodies. Invading organisms or substances are more likely to
cause illness when these concentrations are low. Also, intense exercise during
illness might decrease one’s ability to fight off the infection and increase
the risk of even greater complications.

Predicting the overtraining syndrome
We must remember that the underlying cause or
causes of the overtraining syndrome are not fully known, although it is likely
that physical or emotional overload, or a combination of the two, might trigger
this condition. Trying not to exceed an athlete’s stress tolerance by
regulating the amount of physiological and psychological stress experienced
during training is difficult. Most coaches and athletes use intuition to
determine training volume and intensity, but few can accurately assess the true
impact of a workout on the athlete. No preliminary symptoms warn athletes that
they are on the verge of becoming overtrained. By the time coaches realize that
they have pushed an athlete too hard, it is often too late. The damage done by
repeated days of excessive training or stress can be repaired only by days, and
in some cases weeks or months, of reduced training or complete rest.
Numerous investigators have tried to identify
markers of the overtraining syndrome in its early stages by using assorted
physiological and psychological measurements. A list of potential markers is
provided in the table below. Unfortunately, none has proven totally effective.
It is often difficult to determine whether the measurements obtained are
related to overtraining or whether they simply reflect normal responses to
overload or overreaching training.
Potential
markers of OR, OT and OTS
|
||||
Marker
|
Response
|
Potential
marker for
|
||
Physiological
and psychological
|
OR
|
OT
|
OTS
|
|
HRrest and HRmax
|
Decreased
|
X
|
X
|
|
HRsubmax and VO2submax
|
Increased
|
X
|
X
|
|
Decreased
|
X
|
|||
Anaerobic metabolism
|
Impaired
|
X
|
||
Basal metabolic rate
|
Increased
|
X
|
||
RERsubmax,max
|
Decreased
|
X
|
X
|
|
Nitrogen balance
|
Negative
|
X
|
||
Nerve excitability
|
Increased
|
X
|
||
Sympathetic nervous response
|
Increased
|
X
|
||
Psychological mood states
|
Altered
|
X
|
||
Risk of infection
|
Increased
|
X
|
||
Hematocrit and hemoglobin
|
Decreased
|
X
|
||
Leukocytes and immunophenotypes
|
Decreased
|
X
|
||
Serum iron and ferritin
|
Decreased
|
X
|
||
Serum electrolyte levels
|
Decreased
|
X
|
||
Serum glucose and free fatty acids
|
Decreased
|
X
|
||
Plasma lactate concentration, submax, max
|
Decreased
|
X
|
X
|
|
Ammonia
|
Increased
|
X
|
X
|
|
Serum testosterone and cortisol
|
Decreased
|
X
|
||
ACTH, growth hormone, prolactin
|
Decreased
|
X
|
||
Catecholamines, rest, night
|
Decreased
|
X
|
||
Creatine kinase
|
Increased
|
X
|
||
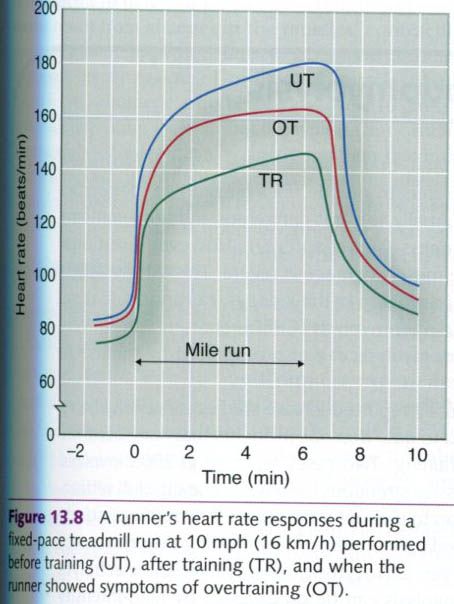
Possibly the best method
to identify the overtraining syndrome is to monitor the athlete’s heart rate
during a standardized workout, such as a fixed-paced run or swim, using a
digital heart rate monitor. The data presented in the figure below illustrate a
runner’s heart rate response during a 1 mi(1.6km) run performed at a fixed pace
of 6 min/mi(3.7 min/km), or 10mph(16km/h). This response was monitored when the
runner was untrained(UT), after the runner had trained(TR), and during a period
when the runner demonstrated symptoms of overtraining syndrome(OT). This figure
allows that heart rate was higher when the runner was in the overtrained state
than when the runner was responding well to training. Similar findings have
been reported for swimmers. Such a test provides a simple and objective way to
monitor training and can possibly provide a warning sign of the onset of the
overtraining syndrome.
Reducing the risk and treating the overtraining
syndrome
Recovery from the
overtraining syndrome is possible with a marked reduction in training intensity
or complete rest. Although most coaches recommend a few days of easy training,
overtrained athletes require considerably more time for full recovery. This
might necessitate the total cessation of training for a period of weeks or
months. In some cases, counseling might be needed to help the athletes cope
with other stress in their lives that might contribute to this condition.
The best way to minimize
the risk of overtraining is to follow periodization training procedures,
alternating easy, moderate, and hard periods of training. Although individual
tolerance varies tremendously, even the strongest athletes have periods when
they are susceptible to the overtraining syndrome. As a rule, one or two days
of intense training should be followed by an equal number of easy training days.
Likewise, a week or two of hard training should be followed by a week of
reduced effort with little or no emphasis on anaerobic exercise.
Endurance athletes(such
as swimmers, cyclists and runners) must pay particular attention to their
carbohydrate intake. Repeated days of hard training gradually reduce muscle glycogen. Unless these athletes consume extra carbohydrate during these
periods, their muscle and liver glycogen reserves can be depleted. As a
consequence, the most heavily recruited muscle fibers are not able to generate
the energy needed for exercise.





0 коментара:
Постави коментар